Firstly, why examine the role of thromboembolic disease in APL when serious bleeding is essentially universal? Thromboembolic episodes are more common than may be appreciated in this setting. The 16% incidence of thromboembolic events observed by Rodriguez-Viega and co-workers is higher than the 12% found in patients with acute myeloid leukemia.5 Furthermore, the major cause of treatment failure in APL is early death and the development of clotting is associated with early death. Early death in APL occurs most frequently during the first 24–48 hours after presentation. Understandably, very few, if any, of such patients are enrolled on clinical trials. Enrollment on a trial would facilitate further insights into thromboembolic events and may pave the way for prevention and therapeutic intervention.
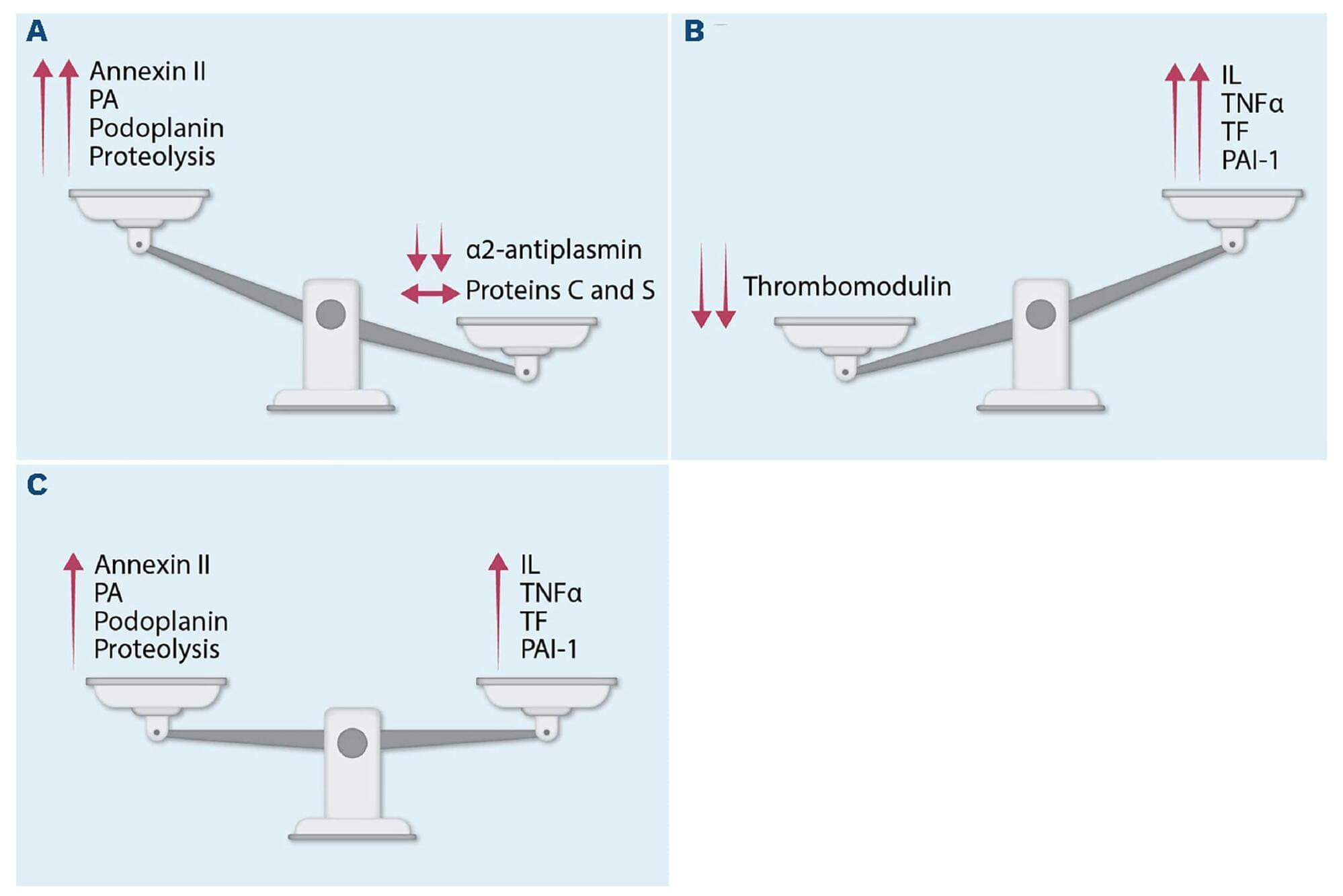
Secondly, why are patients with APL predisposed to develop thrombosis? After all, the disease is infamous for its life-threatening and potentially catastrophic bleeding. This prominent characteristic was recognized by Dr. Leif Hillstad, who is credited with the first description of APL as a distinct clinical entity in 1957.6 Acute promyelocytic leukemia cells are associated with the release of plasminogen activator inhibitor-1, tissue factor, and TNFα. These proteins, together with a decrease in thrombomodulin which functions as an anticoagulant by binding to thrombin, favor the balance towards thromboembolic events7 (Figure 1). Alternatively, with the generation of annexin II, plasminogen activators, and podoplanin, a transmembrane protein which interacts with cell lectin superfamily 2 (CLEC-2) on platelets to induce platelet aggregation and adhesion to lymphatic vessels,8 bleeding is much more commonly present. Furthermore, direct proteolysis of fibrinogen and von Willebrand factor contributes to bleeding. This compilation of processes explains why some patients with APL have bleeding while others have thromboembolic episodes and some have both depending on the balance of procoagulant and anticoagulant proteins. However, bleeding, usually clinically manifested by large ecchymoses on the trunk and extremities, is the major hallmark of the disease.
Finally, how can thromboembolic events in APL be prevented? The most important thing is to maintain a high level of suspicion. The report by Rodriguez-Veiga and co-workers reminds us to be vigilant for the possibility of thromboembolic events in patients with APL. The risk of thrombosis was 1.4% among low-risk patients (presenting WBC 40×109/L), 4.9% for intermediate-risk patients (WBC 10×109/L and platelet count 10×109/L). In contemporary practice, low-and intermediate-risk groups are combined since outcomes among these patients proved to be similar.