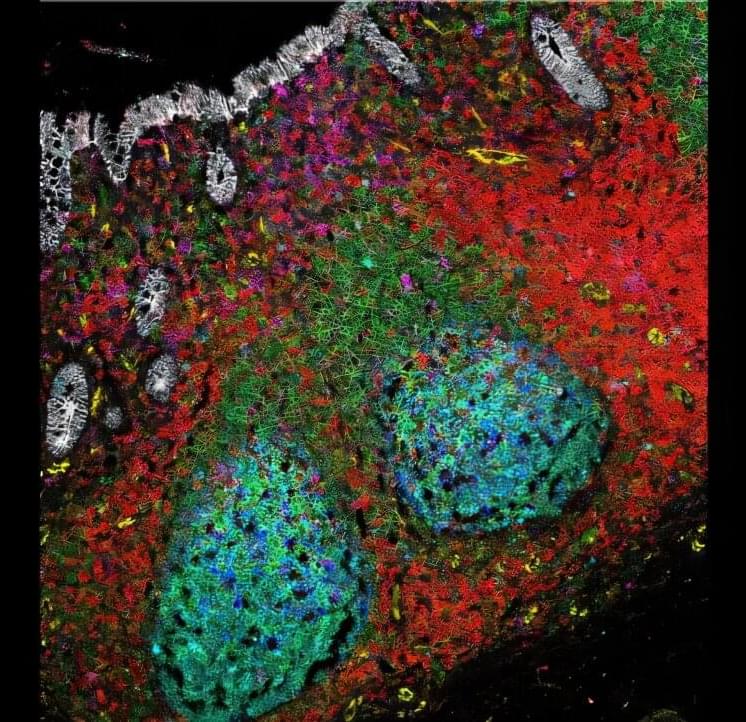
In a new study published in Science Immunology, researchers at King’s College London looked at a type of tissue important for the immune response called gut-associated lymphoid tissue (GALT), which is located within the lining of the gut. Unlike other tissue structures in the gut lining that act as a barrier between the trillions of bacteria in the gut and the rest of the body, GALT actively transports gut microbes into the body. By doing this, GALT activates immune responses that help maintain a stable relationship with beneficial gut bacteria.
Typically, when the body encounters microbes, it triggers inflammation, sending immune cells to the affected area to fight the pathogen. However, GALT behaves differently. Despite its close and consistent interaction with microbes, GALT does not become inflamed.
To understand how GALT achieves this, the team mapped the interactions and locations of immune cells in GALT. They also looked at how these interactions changed in ulcerative colitis—an inflammatory bowel disease in which parts of the large bowel become swollen, inflamed and ulcerated. According to Crohn’s & Colitis UK, at least 1 in every 233 people in the U.K. have ulcerative colitis. The condition can significantly affect quality of life. Previous research has linked GALT in the appendix to ulcerative colitis.