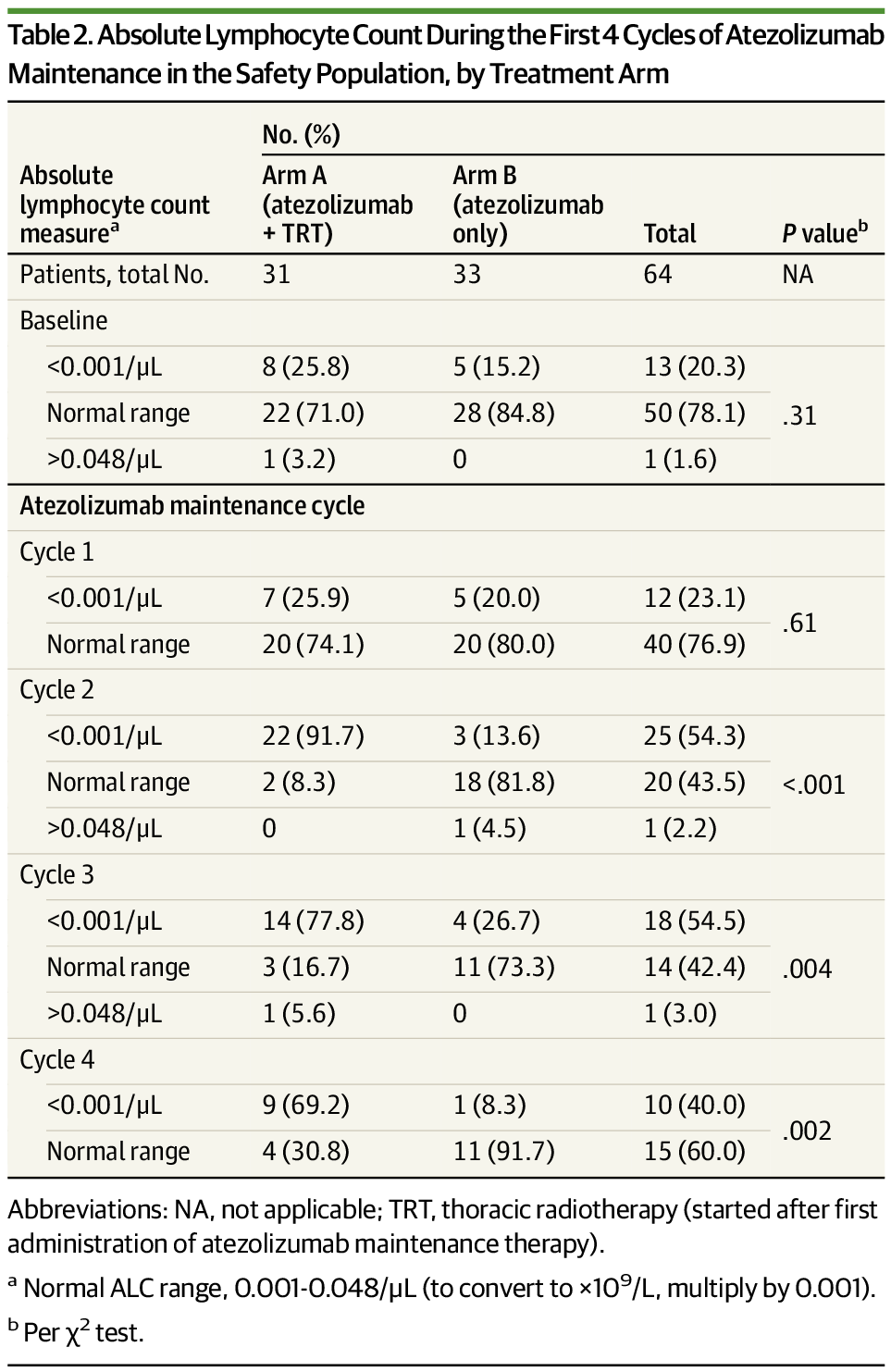
This phase 2 randomized clinical evaluates whether combining consolidative thoracic radiotherapy with immunotherapy maintenance in extensive-stage small cell lung cancer overall survival (OS), progression-free survival (PFS), or safety.
AI chatbots can describe reality in words, but don’t truly understand cause and effect in the real world. Now, a fresh kind of machine intelligence that does just that is emerging
Karl Marx knew the future. Not suspected it. Knew it. The revolution was inevitable, and history had a timetable.
Silicon Valley talks the same way now.
Technology has a direction, the exponential is its engine, and the singularity is its destination. You can slow the train, they say, but you cannot stop it.
I spent seventeen years and 300+ interviews taking that story seriously. I was a believer. In 2006 it blew my mind, and I built half a life on it.
Today I am the skeptic. And I have finally written down exactly why I turned.
Because when you strip the singularity down to its engine, it is not a forecast at all. It is a religion, and I can show you the receipts, using Ray Kurzweil’s own diagram to do it.
This is not an attack from the outside. It is a confession from someone who used to preach it.
And there is an important reason this doesn’t necessarily mean we’re headed for a “dead Internet.”
Built on one of the world’s largest networks, Precursor is the only defense of its kind to replace disruptive checkpoints to stop evasive bots without slowing down users
SAN FRANCISCO—(BUSINESS WIRE)— Cloudflare, Inc. (NYSE: NET), the leading connectivity cloud company, today announced the general availability of Precursor, a next-generation, continuous behavioral validation engine for bot management. Built directly on Cloudflare’s edge, Precursor runs seamlessly inside web browsers to monitor entire user sessions in order to detect bot automation. Unlike traditional, static CAPTCHAs, it analyzes ongoing interactions in real time to catch advanced bots, improving detection precision without interrupting legitimate users.
For the first time, automated bot traffic has eclipsed human activity on the Internet, now generating roughly 57% of all web requests. This milestone emphasizes a seismic evolution from an Internet built for human clicks to a digital landscape now dominated by AI agents. For organizations and everyday consumers, this means that legacy defenses are blind to a new breed of automated threats that drive up infrastructure costs, manipulate inventory, and compromise data. While a modern bot can easily fake a single action to pass a one-time security check, replicating an entire human journey remains a massive engineering hurdle. To protect the integrity of the global Internet, organizations must move away from static, point-in-time defenses and embrace continuous behavioral validation—analyzing telemetry across an entire session to unmask automated imposters trying to blend into the crowd.

WASHINGTON — The company that developed a spacecraft to boost the orbit of a NASA observatory says it is making progress in recovering from its own spacecraft’s problems.
In a social media post last week, Katalyst Space Technologies said it had slowed the spin of its Link spacecraft, which had entered what the company said on July 28 was a “multi-axis spin” because of technical issues encountered during post-launch commissioning.
“LINK was spinning at approximately 9 degrees per second when recovery operations began,” the company stated. “The team has since reduced the spacecraft’s body rate to 1.47 degrees per second, where it will remain while the team prepares for the next phase of the mission.”
Samsung didn’t promote from within to lead RX’s strategy — it hired Executive Vice President Lee Dongkun, who previously directed robotics strategy at Hyundai Motor Group, the parent of Boston Dynamics, and who oversaw development of the electric Atlas humanoid and Spot quadruped during Hyundai’s push to commercialize both. That hire, paired with Samsung’s Rainbow Robotics subsidiary already commercializing the RBY1 wheeled dual-arm platform and developing HUBO bipedal prototypes, signals a company assembling deployment expertise, not just research capability. See our coverage of Unitree’s TIME cover hiding a 9% industrial deployment problem for how deployment expertise, not funding or hype, is the scarce resource across this entire sector right now.
Samsung’s in-house robots strategy also extends to components most competitors buy from third parties: the company is developing its own actuators using motor technologies adapted from home appliances, an unusual but financially logical move for a company that already runs enormous consumer-electronics manufacturing lines. Owning that layer reduces both cost and dependency on the same small set of actuator suppliers every other humanoid maker competes for.
⚠ Fiction — composite scenario, not a real event: A robotics analyst covers Samsung’s RX division purely as a Tesla and Unitree competitor, publishing a forecast comparing unit shipment targets. Two years later, Samsung has shipped fewer finished humanoids than expected — but its foundry chip revenue from robotics customers across five different manufacturers has quietly become a bigger business line than the humanoid unit itself, exactly the outcome the shipment-focused forecast never modeled.

Results from a small clinical trial suggest it may be possible to reduce the risk of dementia by eating during fewer hours of the day. The pilot study, which involved a weight-loss program for older women with overweight or obesity, showed modest cognitive improvements among those who limited their daily eating window instead of just reducing their calorie intake.
“Losing weight alone will ward off some of the aging-related cognitive decline, and these data suggest that there may be additional benefits if you stop eating four hours before going to sleep and reduce food intake to 8–9 hours per day, compared with the usual eating window of 12 hours per day,” said Sue Shapses, Ph.D., RD, DFASN, professor at Rutgers University and Rutgers-RWJ Medical Center and the study’s principal investigator.
Shapses’ group will present the findings at NUTRITION 2026, the flagship annual meeting of the American Society for Nutrition, held July 25–28 in National Harbor, Maryland, just outside Washington, D.C.

Situational Awareness may have had to sell off the majority of its public portfolio last month, but the AI-focused hedge fund is still making some big bets.
This week, the fund invested $400 million into Source Foundry, a startup founded by Stanford researchers aiming to make chip manufacturing faster and cheaper, according to The Wall Street Journal. That brings its total investment in Source Foundry to $500 million.
Situational Awareness was founded by Leopold Aschenbrenner, a former OpenAI researcher in his mid-twenties who had no trading experience when he launched the fund in 2024. Early returns were reportedly strong, but the fund faced steep losses in recent months amidst the decline in AI infrastructure stocks.

A study of 4,818 middle-aged and older Chinese adults found that higher light BioAge was associated with greater risks of cognitive impairment, episodic memory decline, and reduced mental intactness. The simple measure, based on age, creatinine, glucose, and CRP, added modest predictive information but requires further validation before clinical use.