Scientists expected that wiping out most of the skin’s fibroblast population would shut down stem cell growth. Instead, the skin barely flinched.
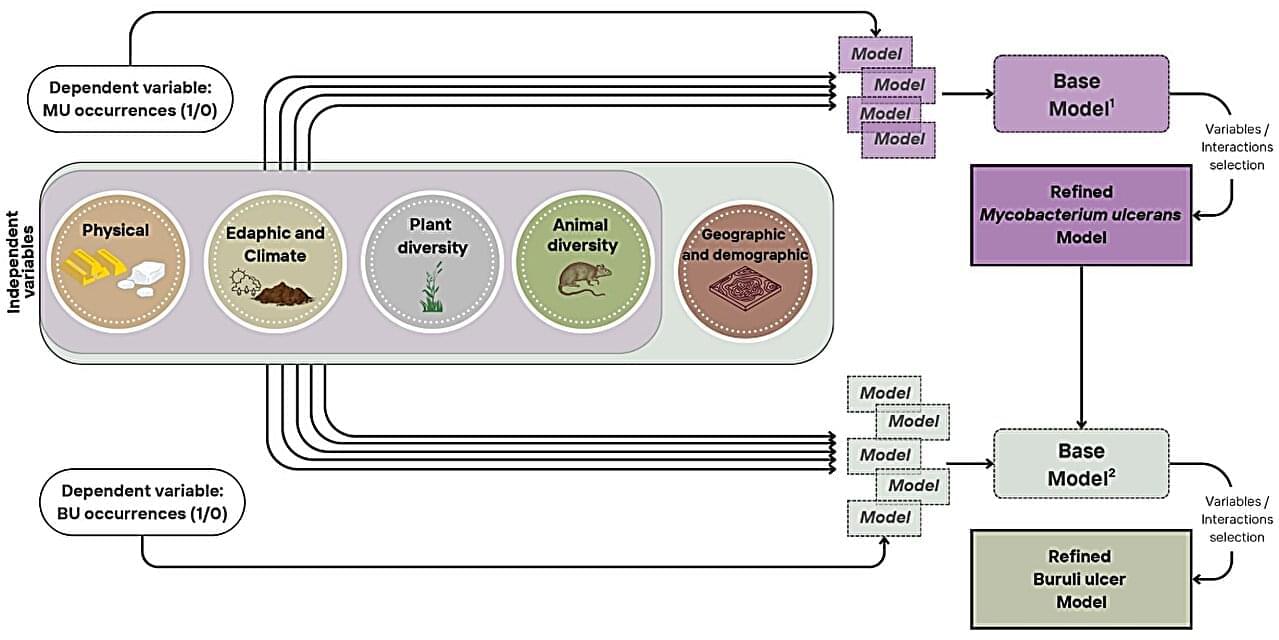
When the COVID-19 pandemic shut down international travel in 2020, Michigan State University researcher Eric Benbow faced a problem. A $2.5 million research project designed to study an environmental pathogen in South America was suddenly on hold. With fieldwork canceled and uncertainty surrounding when travel might resume, Benbow and his collaborators needed a new plan.
That unexpected detour led to a surprising discovery—and new insights into a disease that has puzzled scientists for decades.
In their study published in Communications Medicine, the international team of researchers examined the environmental and human factors that influence the distribution of Buruli ulcer, a neglected tropical disease caused by the bacterium Mycobacterium ulcerans. The work helps explain how ecosystems, climate, land use and human activities interact to shape disease risk.

Every person’s DNA tells a unique story. To unlock the full potential of genetic research, scientists need tools that reflect the complexity of the people they study.
Researchers at Baylor College of Medicine and Texas Children’s Duncan Neurological Research Institute (Duncan NRI) have developed a new computational method that enables scientists to more accurately identify genetic changes linked to disease by accounting for the ancestry and family relationships found in real-world populations.
Published in Nature Genetics, the new approach, called Tractor-Mix, addresses a longstanding challenge in genetic research. Many existing methods struggle to accurately analyze people whose DNA reflects ancestry from more than one ancestral population, as well as relatives participating in the same study. As a result, researchers often must simplify their data or exclude participants altogether.
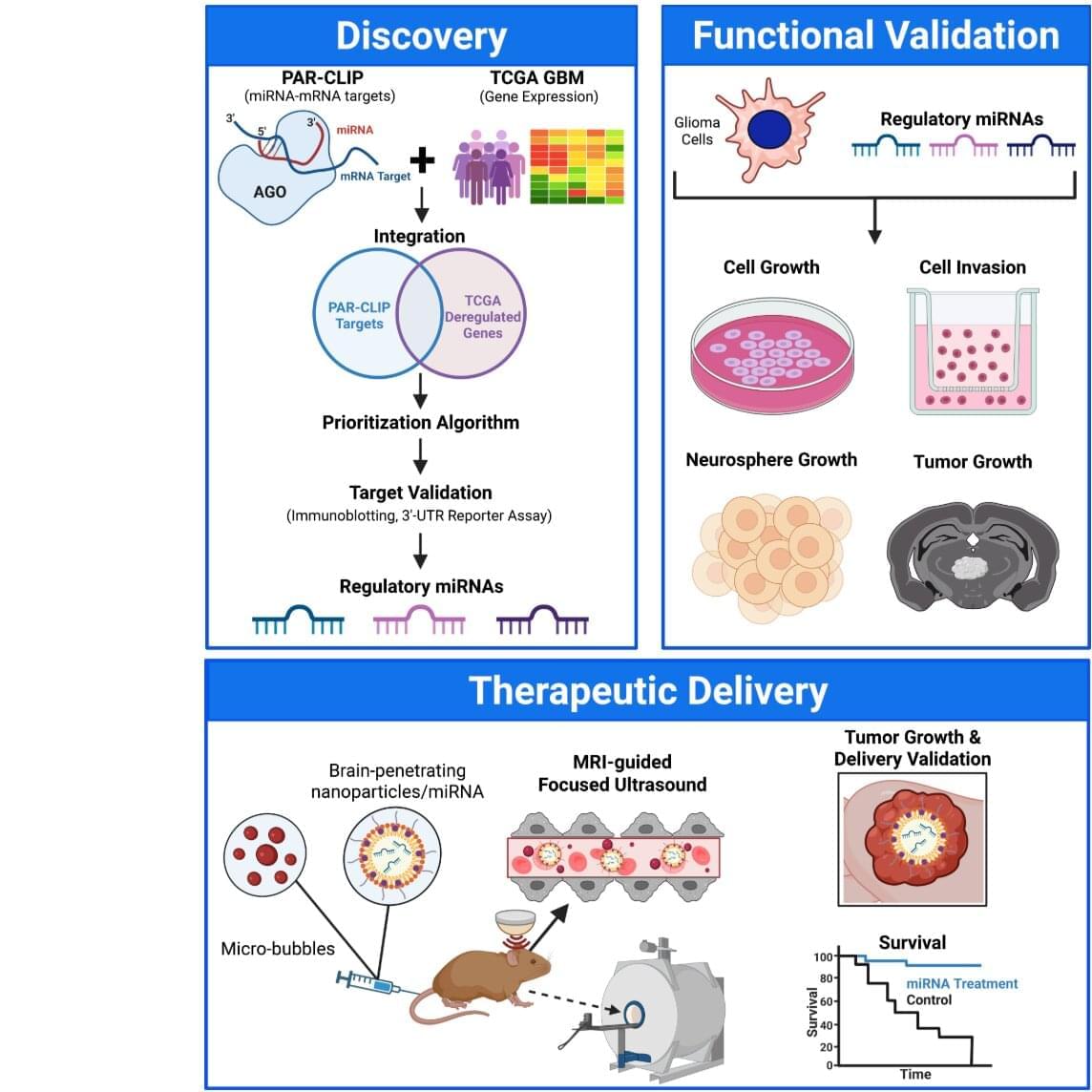
University of Virginia Comprehensive Cancer Center scientists have developed a promising new experimental approach to targeting glioblastoma, the most common and deadliest brain cancer. The approach could overcome many of the limitations of treatments using existing drugs.
UVA’s Roger Abounader, MD, Ph.D., and colleagues have identified “microRNAs” that can simultaneously suppress multiple malfunctioning genes responsible for glioblastoma’s formation and growth. The scientists use a combination of brain-penetrating nanoparticles, focused ultrasound waves and microbubbles to deliver the miRNAs through the brain’s natural protective barrier—a barrier that typically blocks treatments for tumors and neurodegenerative diseases. The study is published in the Journal of Clinical Investigation.
“This new approach could help target numerous molecules that promote cancer growth, including those for which no drugs exist, at the same time to achieve better therapies,” said Abounader, a professor at UVA’s School of Medicine, Department of Microbiology, Immunology and Cancer Biology, Comprehensive Cancer Center and Center for RNA Science and Medicine. “We are hoping to translate our findings into future clinical trials for patients with glioblastoma and other brain tumors.”
Why do cancers develop differently in different people—even when they are exposed to the same risk factors? An international research group, including the German Cancer Research Center (DKFZ), has demonstrated in mice that an organism’s genetic makeup significantly influences the course of cancer development.
The findings, published in Nature, provide new insights into the earliest stages of tumor development and could, in the long term, represent an important step toward more precise, personalized cancer medicine.

In creating a comprehensive, AI-enabled research agent for the biomedical sciences, Stanford University researchers hope to speed innovation by eliminating the tedium of scientific legwork. Biomni, an AI-powered, multiskilled biomedical research agent, is no mere chatbot. It is a full-fledged “co-scientist” capable of designing and developing complex research workflows, said Jure Leskovec, the Alfred and Rebecca Lin Professor and professor of computer science in the School of Engineering and senior author of the paper introducing Biomni in the journal Science.
“If you think of an agent as a carpenter, a carpenter without tools is just a carpenter who can talk,” Leskovec said, explaining what sets Biomni apart from popular generative AI chatbots. “With Biomni, we give the carpenter a set of tools, so it can build.”
Born for impact Biomni was born from the notion that, when working with an AI agent, a scientist should be able to describe a research problem in simple, natural language. With that in mind, the researchers designed Biomni to read the literature, form hypotheses, choose datasets and tools, write code, interpret results and suggest next-stage experiments in a complete research workflow.
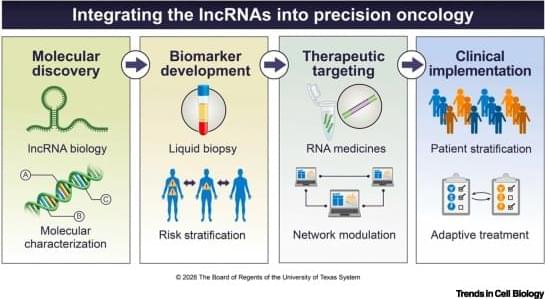
Long noncoding RNAs (lncRNAs) regulate the tumor microenvironment (TME), yet their cell-intrinsic roles within immune populations of the TME remain underappreciated. In this review, we shift focus from the cancer cell to the immune compartment, systematically reviewing how immune cell-intrinsic lncRNAs govern CD8+ T cell exhaustion, CD4+ T cell polarization, NK cell cytotoxicity, dendritic cell antigen presentation, and macrophage inflammatory programming. We highlight lncRNAs that function as molecular switches—tipping immune cells between antitumor effector and immunosuppressive states—and examine how exosomal lncRNAs extend these regulatory circuits across cellular boundaries within the TME.
When the iconic rock band Queen asked, “Who wants to live forever?” the question was rhetorical, but for many people, the answer was “Yes”
Well, a new study suggests immortal life may be scientifically impossible, even if we somehow found the perfect anti-aging medicine.
If scientists managed to overcome every other aspect of aging, humans still couldn’t live forever, the new research shows. Random DNA mutations would continue accumulating in our cells until the body could no longer function.
{kind=link}