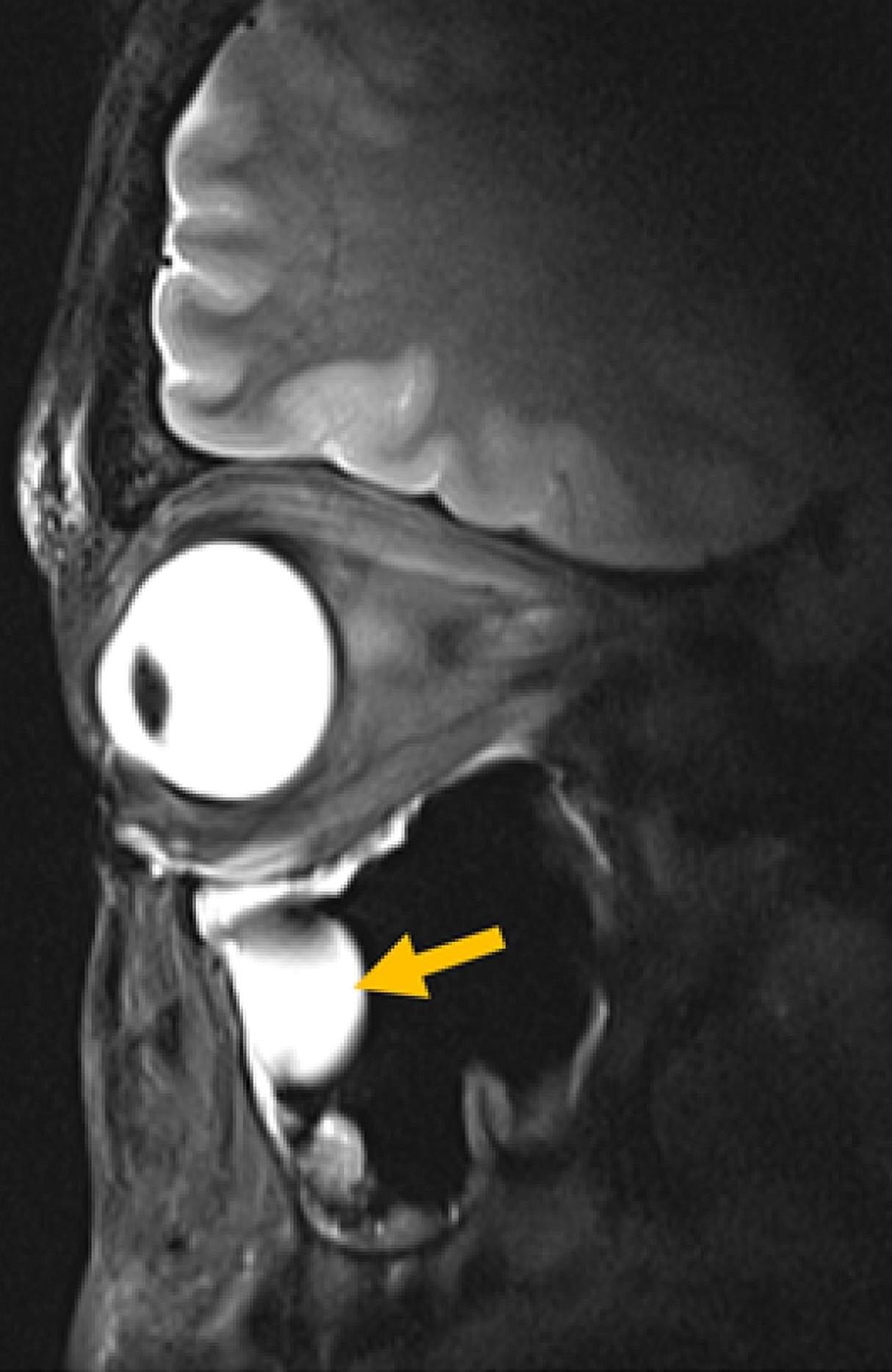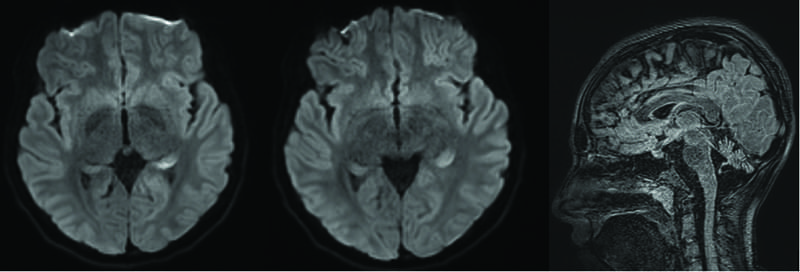
Imaging results also demonstrated marked cerebellar atrophy, which is a recognized feature of CACNA1A-related disorders.13 Although the timing and progression of this abnormality are uncertain because UL last underwent brain imaging in infancy, the need for structured evaluation throughout development is clear. We also noted asymmetric fluid-attenuated inversion recovery signal in the left mesial temporal lobe, which was believed to be most consistent with postictal edema given the known overlap between CACNA1A channelopathies and seizure susceptibility.
This case highlights the diagnostic uncertainty of CACNA1A-related hemiplegic migraine and emphasizes the need for early exclusion of stroke and seizure, in addition to timely escalation of preventive therapy when symptoms persist beyond their typical timeframes. The clinical response to an increased acetazolamide dose, initiation of verapamil, and corticosteroids for cerebral edema provides additional support for current recommendations in a field where high-quality evidence remains limited.