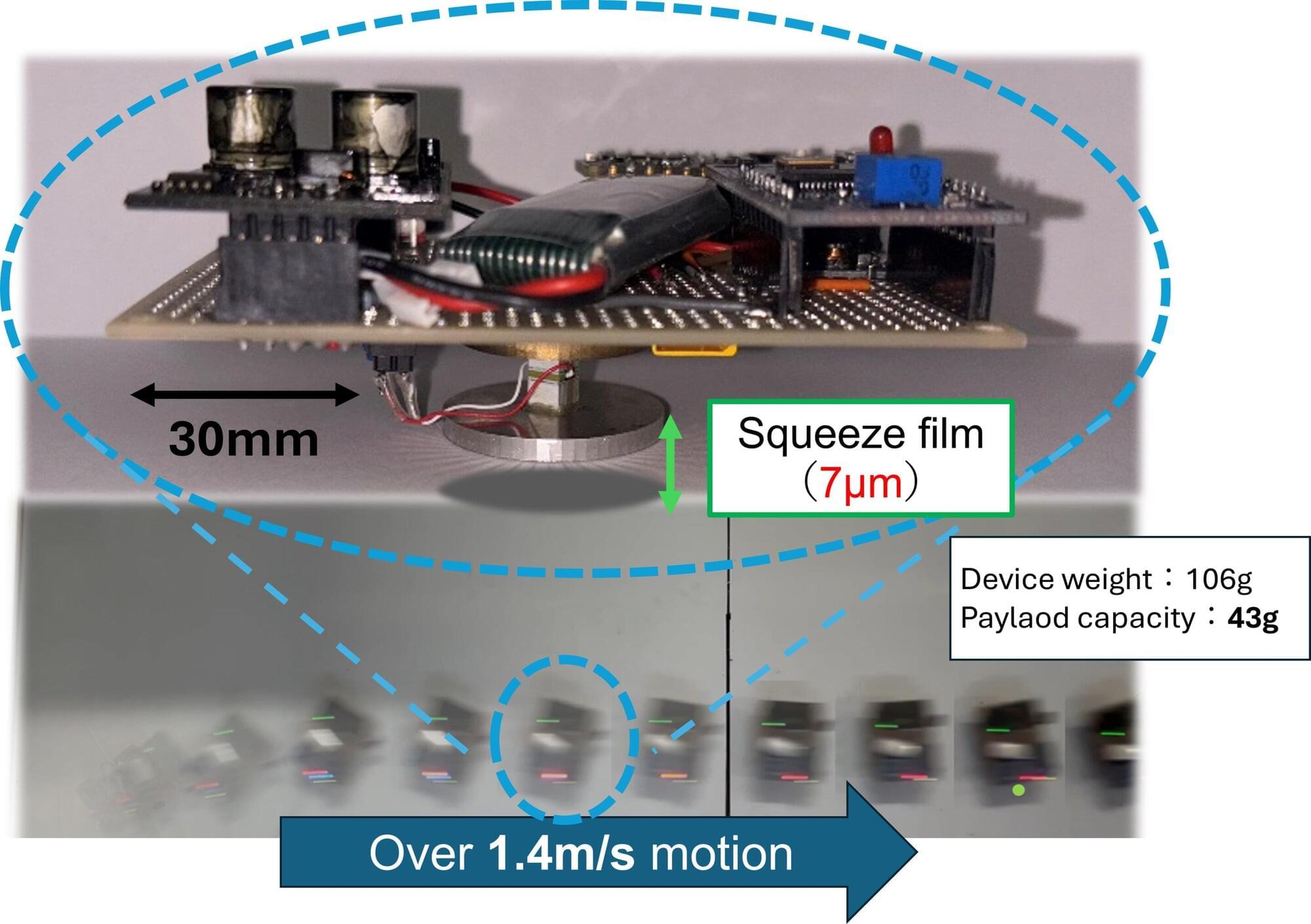
Advances in technology have led to the miniaturization of many mechanical, electronic, chemical and biomedical products, and with that, an evolution in the way these tiny components and parts are transported is necessary to follow. Transport systems, such as those based on conveyor belts, suffer from the challenge of friction, which drastically slows the speed and precision of small transport.
Researchers from Yokohama National University addressed this issue by developing an untethered levitation device capable of moving in all directions. The frictionless design allows for ultrafast, agile movement that can prove to be very valuable in machine assembly, biomedical and chemical applications via contactless transport.
Genetic pet customization, designer pets 2050, futuristic pets, custom animal genetics, dna pet editing, crispr pets, designer dogs future, genetic engineering pets, bioengineered animals, create your own pet species, pet dna editing, designer cats 2050, genetic modified pets, custom pet labs, crispr cats, crispr dogs, futuristic pet ownership, biotechnology pets, glow in the dark pets, designer parrot genetics, genetic pet store future, engineered pets 2050, synthetic pets, build your own pet, dna modified animals, pet cloning future, futuristic pet breeds, genetic pets documentary, custom pets 2050, future animal technology, crispr pet design, genetically engineered pets, future dog breeds, custom parrot species, lab created pets, designer fish dna, genetic pet creation, future pet shops, crispr technology pets, bio pet labs future, create hybrid pets, animal dna editing, futuristic pet designs, design your own pet future, genetically customized animals, pet modification labs, genetic breeding future, synthetic biology pets, dna pet labs, engineered pet genetics, future hybrid pets, bioluminescent pets, pet dna science, designer turtles 2050, futuristic exotic pets, pet cloning labs, genetically programmed pets, dna modified species, designer hybrid animals, future of pets, biotechnology dogs, crispr engineered pets, pet dna modification, hybrid pets future, lab made pets, designer parrots, glowing pets dna, futuristic animal science, genetic modification animals, future pets prediction, dna engineered animals, custom pet species, crispr biotechnology pets, synthetic animal breeds, futuristic family pets, engineered exotic pets, dna edited dogs, glow in the dark cats, crispr futuristic pets, genetically designed pets, dna engineered cats, hybrid pet genetics, genetic evolution pets, pet dna design, engineered turtles, pet biotechnology future, futuristic pets science, genetic designer animals, crispr engineered dogs, dna pet programming, designer bio pets, dna hybrid animals, genetic dog breeds future, biotechnology cat design, future pet customization, dna edited parrots, bioengineering pets, custom pet dna science, crispr engineered animals, future designer pets 2050, dna reprogrammed animals, pet biotechnology industry, genetic engineered parrots, engineered hybrid dogs, futuristic pet labs, dna custom pets, genetic engineered cats, crispr glowing pets, biotechnology future pets, genetic science pets, future pet dna editing, lab created exotic pets, dna modified exotic animals, engineered pet cloning, futuristic pet market, genetic engineered hybrid pets, future animal dna science, biotechnology glowing pets, synthetic dna animals, futuristic pet lovers, pet dna labs 2050, engineered pet stores, custom dna pets future, future glowing cats, crispr glowing dogs, bioengineered hybrid pets, designer dna parrots, pet dna bio labs, futuristic exotic pet design, dna animal modification, engineered mini elephants, genetic designed turtles, futuristic pets 2070, dna modification in pets, custom engineered pets, biotechnology hybrid species, genetic glowing animals, pet dna engineering labs, designer pet hybrids, dna created exotic pets, future pet technology, genetically edited pets, bio custom pet stores, engineered pet dna future, dna glowing parrots, designer genetic cats, future biotechnology pets, crispr custom pets, engineered family pets, dna hybrid parrots, future pet science documentary, pet dna labs future, engineered dog species, future bioengineered animals, pet cloning 2050, custom glowing pets, biotechnology engineered cats, crispr glowing animals, genetically designed parrots, futuristic pet lab science, dna engineered turtles, designer animal dna, engineered futuristic pets, pet biotechnology predictions, dna designer pets, genetic engineered glowing animals, future pet design 2050, dna bioengineered cats, futuristic hybrid pet market, crispr engineered exotic pets, engineered glowing dogs, dna glowing exotic pets, biotechnology pet predictions, futuristic designer pets science, engineered pet bio labs, dna exotic animal design, genetic glowing turtles, future engineered animal species, custom dna exotic pets, crispr designed parrots, engineered glowing cats, futuristic pet dna bio labs, biotechnology glowing dogs, dna engineered glowing parrots, engineered pet biotechnology labs, custom dna glowing pets, future engineered exotic animals, genetic designed dogs, crispr engineered glowing cats, future biotechnology exotic pets, engineered hybrid parrots, dna glowing turtles, engineered exotic pet labs, genetic bio engineered animals, futuristic dna pet predictions.
Take note of the name: ReHMGB1. A new study pinpoints this protein as being able to spread the wear and tear that comes with time as it quietly travels through the bloodstream. This adds significantly to our understanding of aging.
Short for reduced high mobility group box 1, ReHMGB1 triggers senescence in cells, permanently disabling them. It doesn’t just do this locally; it can send damaging signals throughout the body, particularly in response to injuries or disease.
“An important question in aging research is why senescent cells increase with age,” write the study authors, led by researchers from the Korea University College of Medicine.
A new study, led by researchers at Children’s Hospital of Philadelphia (CHOP), identified tiny pieces of messenger RNA that are missing in pediatric high-grade glioma tumors but not in normal brain tissues. Preclinical research indicates that these missing RNA fragments can make difficult-to-treat tumors more responsive to immunotherapy. The findings were recently published in the journal Cell Reports.
One of the biggest challenges facing cancer research is the need to find safe and effective therapies for the most aggressive types of brain tumors. Adoptive immunotherapies with CAR-T cells are promising; however, they often also target healthy cells, which share most surface proteins with cancerous cells. While this collateral damage might be tolerable in patients with certain types of blood cancer, in the brain, wiping out healthy neurons is unacceptable. This means that deep knowledge of gene expression patterns exclusive to tumor cells is critical.
A potential means of discovering new therapeutic targets for brain tumors may lie in alternative splicing, a process whereby a single gene produces multiple proteins by rearranging exons, the building blocks of messenger RNA, in different combinations. Researchers suspected that splicing in glioma cells may differ from splicing in normal brain cells, which could help devise new therapeutic interventions.
Synthetic cells are artificial constructs designed to mimic cellular functions, offering insights into fundamental biology, as well as promising impact in the fields of medicine, biotechnology, and bioengineering. In this perspective, the authors highlight major scientific hurdles, such as the integration of functional modules by ensuring compatibility across diverse synthetic subsystems, and propose strategies to advance the field.
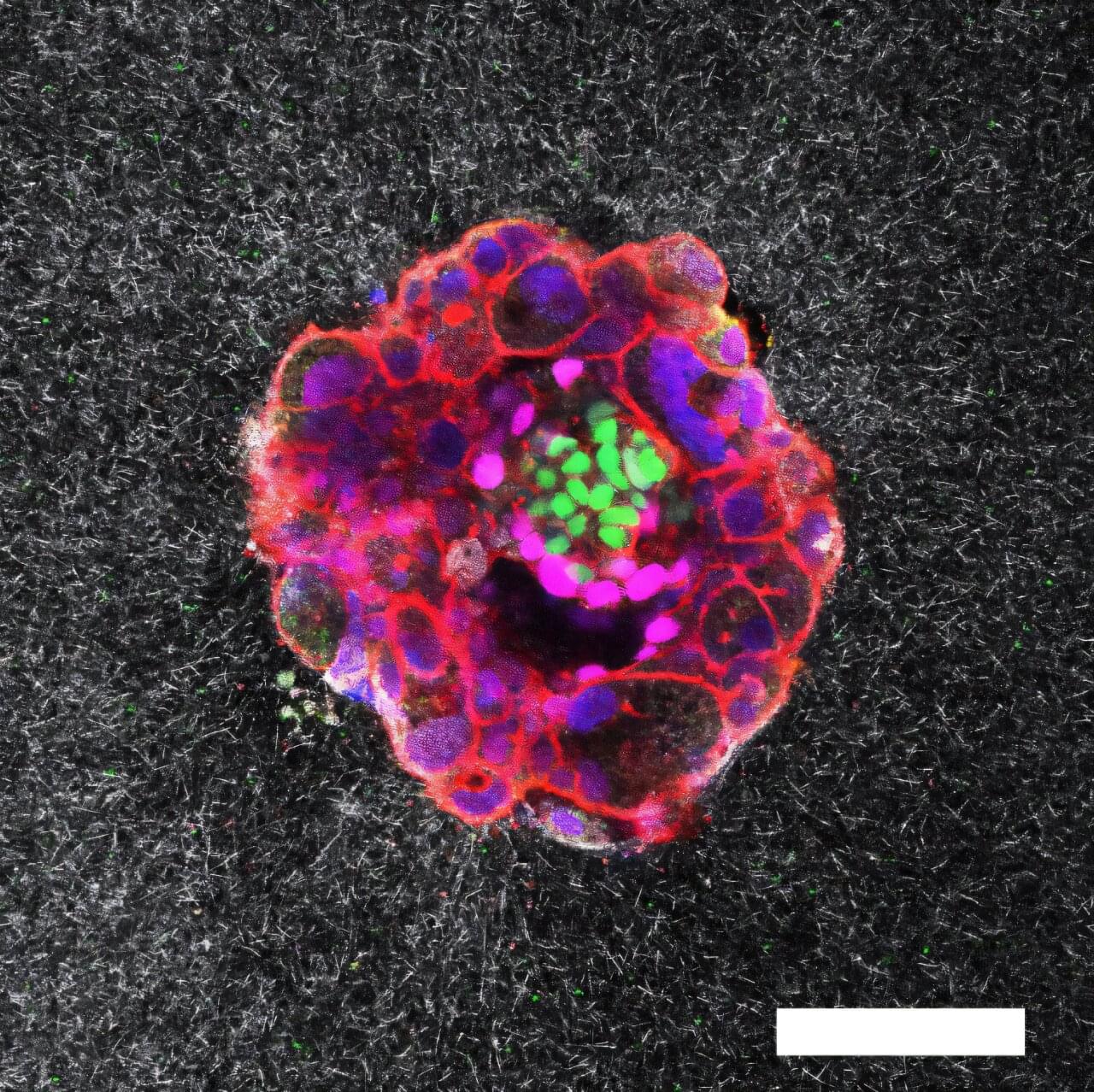
Researchers at the Institute for Bioengineering of Catalonia (IBEC) in collaboration with the Dexeus University Hospital have captured unparalleled images of a human embryo implanting. This is the first time that the process has been recorded in real time and in 3D.
Hospital Clínico San Carlos in Madrid-led research reports that intermittent theta-burst transcranial magnetic stimulation (TMS) paired with language therapy over six months was associated with positive outcomes in primary progressive aphasia (PPA). Improvements included less decline in regional brain metabolism and improvements in language abilities, functional independence, and neuropsychiatric symptoms.
Primary progressive aphasia is a neurodegenerative clinical syndrome with insidious onset characterized by prominent speech and/or language impairment. It is a syndrome that can be the mode in which common causes of dementia, Alzheimer’s disease and frontotemporal degeneration are initially present.
According to current international consensus criteria, three variants are recognized: nonfluent/agrammatic, semantic, and logopenic. Speech-language intervention has proven to be beneficial.
A new generation of CRISPR technology developed at UNSW Sydney offers a safer path to treating genetic diseases like sickle cell, while also proving beyond doubt that chemical tags on DNA—often thought to be little more than genetic cobwebs—actively silence genes.
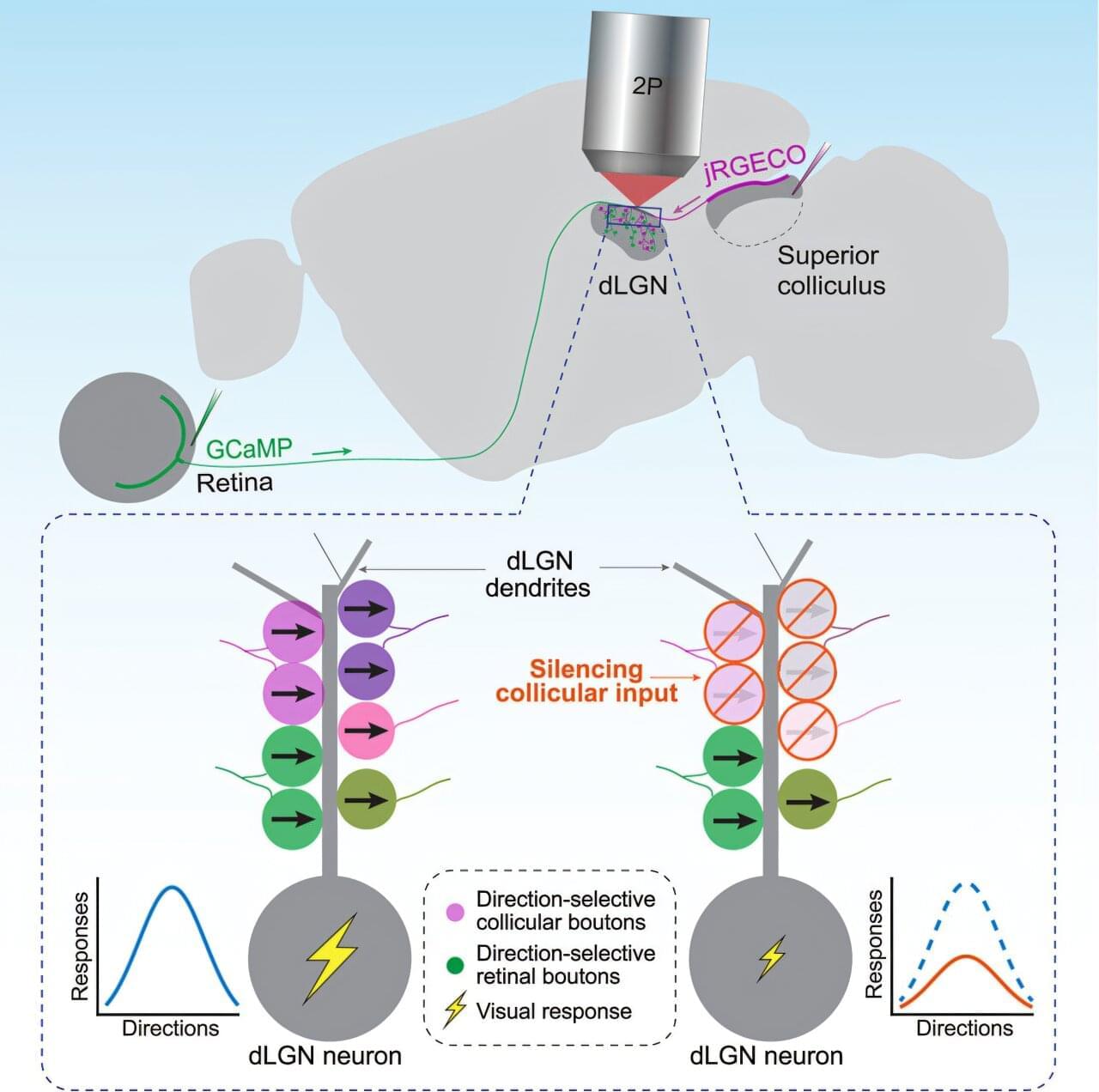
When you see something—a tree in your backyard, say, or the toy your toddler hands you—that visual information travels from your retinas to your brain. And like a train stopping at stations along its route, the information pauses at particular regions of the brain where it’s processed and sent along to its next location.
A region called the visual thalamus has been thought to be primarily a relay, simply directing visual information to its next area. But a new study published in Neuron finds that the thalamus actually integrates additional information from other brain regions and reshapes the information it sends along to the brain cortex.
Liang Liang, Ph.D., assistant professor of neuroscience at Yale School of Medicine (YSM) and senior author of the study, suspected the thalamus might be doing more than it had been given credit for.
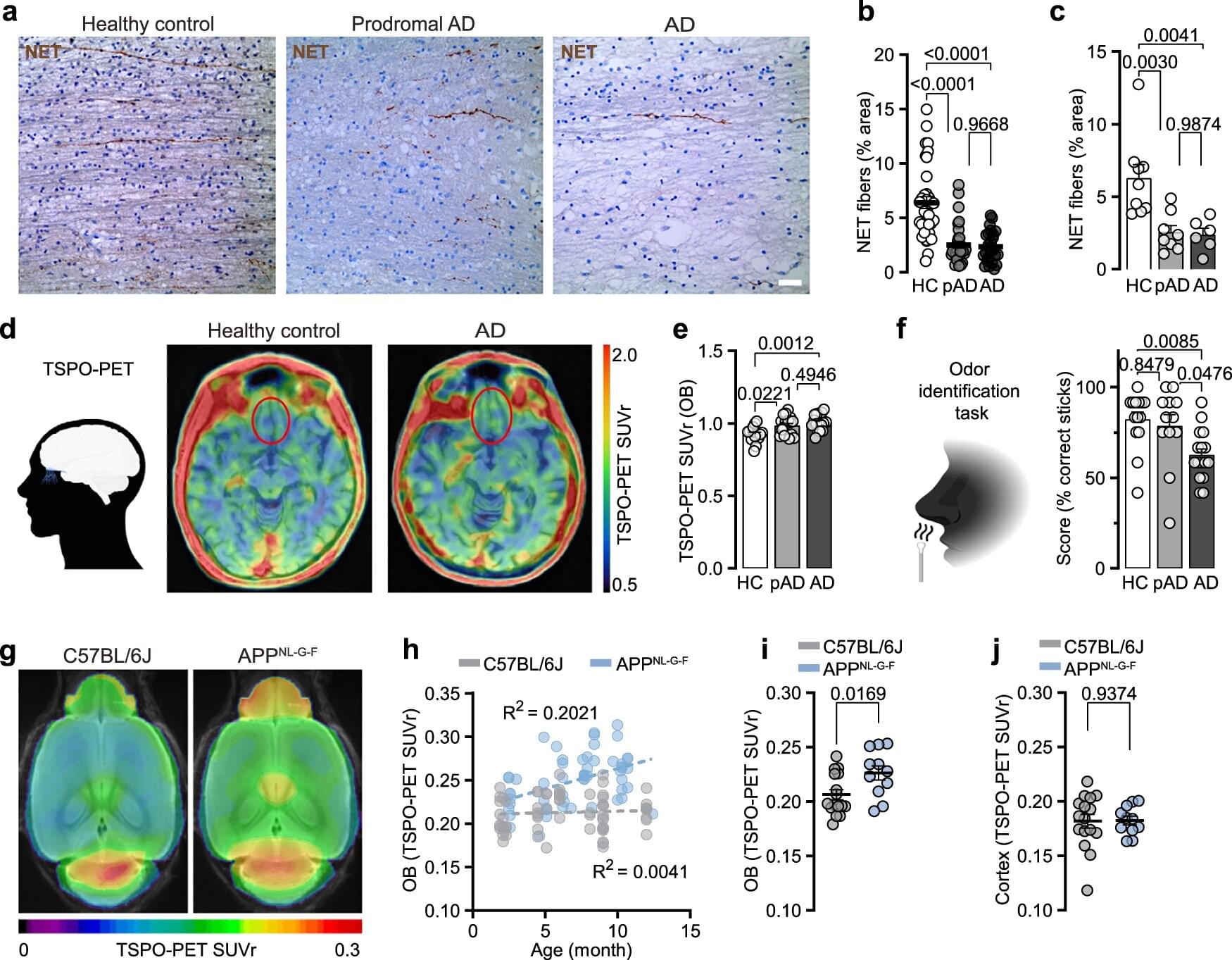
A fading sense of smell can be one of the earliest signs of Alzheimer’s disease even before cognitive impairments manifest. Research by scientists at DZNE and Ludwig-Maximilians-Universität München (LMU) sheds new light on this phenomenon, pointing to a significant role for the brain’s immune response, which seems to fatally attack neuronal fibers crucial for the perception of odors.
The study, published in Nature Communications, is based on observations in mice and humans, including analysis of brain tissue and so-called PET scanning. These findings may help to devise ways for early diagnosis and, consequently, early treatment.
The researchers came to the conclusion that these olfactory dysfunctions arise because immune cells of the brain called “microglia” remove connections between two brain regions, namely the olfactory bulb and the locus coeruleus.



{kind=link}
{kind=link}
{kind=link}