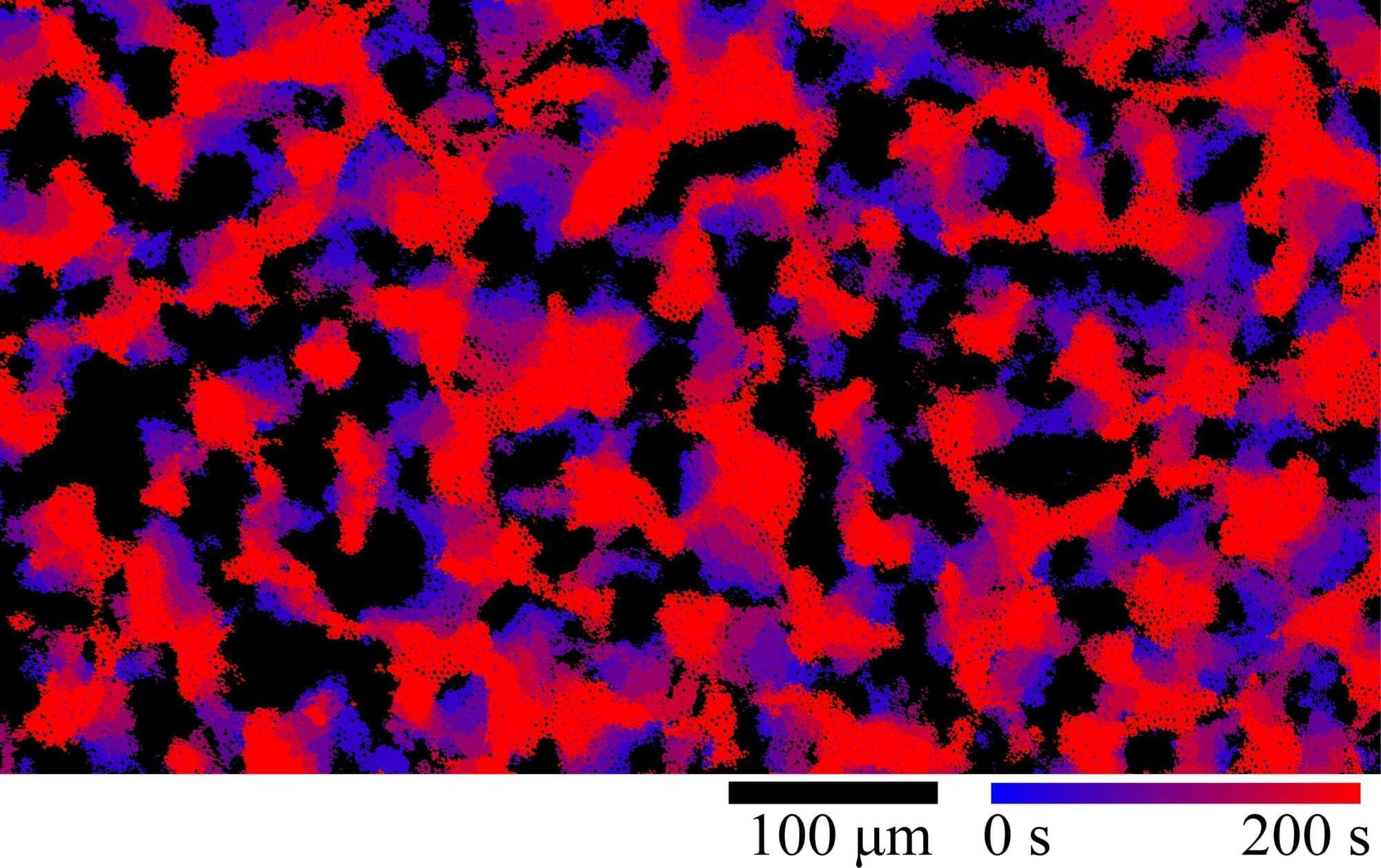
Skyrmions—essentially magnetic vortices—represent a promising approach in spintronics; in the future, they could serve as components in storage media or computers, potentially complementing established CMOS technologies. Researchers at Johannes Gutenberg University Mainz (JGU) have now visualized the interaction of antiferromagnetic skyrmions for the first time and shown that antiferromagnetic skyrmions move reproducibly along straight trajectories aligned with the driving electric current.
“Our results establish a quantitative framework for the interactions of antiferromagnetic skyrmions. In doing so, they pave the way for spintronic devices based on large numbers of skyrmions,” said Mona Bhukta from the research group of professor Mathias Kläui at the JGU Institute of Physics. The researchers published their findings today in the journal Nature Physics.