A breakthrough in fluorescence microscopy has been achieved by the research group of Ralf Jungmann at the Max Planck Institute of Biochemistry (MPIB) and Ludwig-Maximilians-Universität (LMU) Munich. The team developed Resolution Enhancement by Sequential Imaging (RESI), a revolutionary technique that enhances the resolution of fluorescence microscopy down to the Ångström scale. This innovation is poised to usher in a paradigm shift in our approach to study biological systems with thus far unprecedented detail.
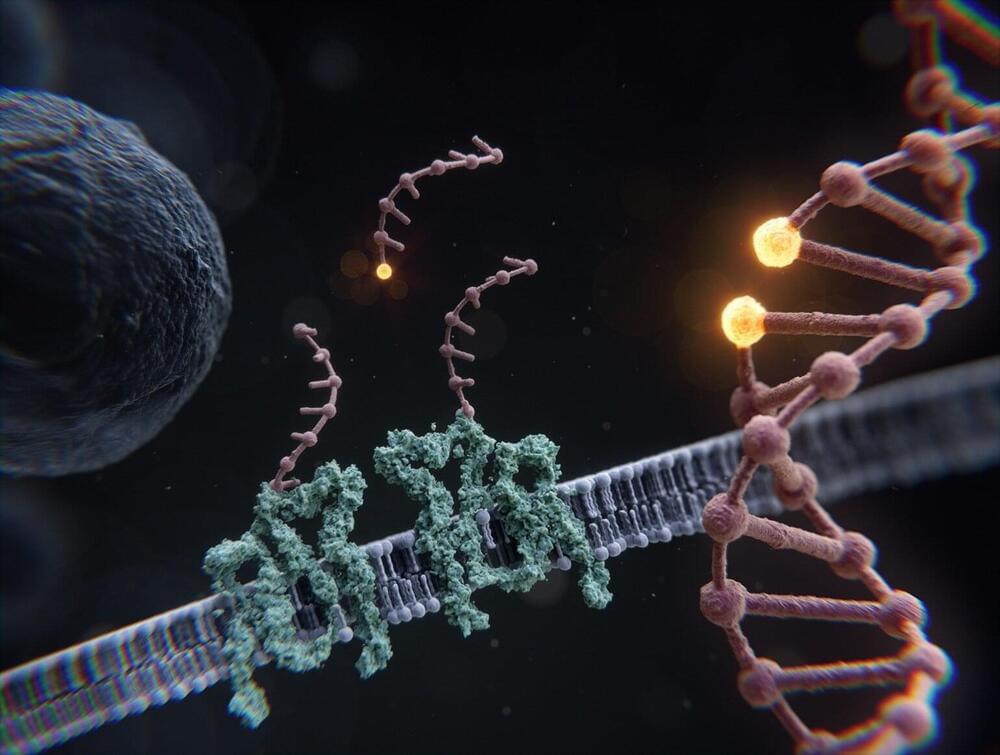
Cells, the fundamental units of life, contain a plethora of intricate structures, processes and mechanisms that uphold and perpetuate living systems. Many cellular core components, such as DNA, RNA, proteins and lipids, are just a few nanometers in size. This makes them substantially smaller than the resolution limit of traditional light microscopy. The exact composition and arrangement of these molecules and structures is thus often unknown, resulting in a lack of mechanistic understanding of fundamental aspects of biology.
In recent years, super-resolution techniques have made leaps and bounds to resolve many sub-cellular structures below the classical diffraction limit of light. Single molecule localization microscopy, or SMLM, is a super-resolution approach that can resolve structures on the order of ten nanometers in size by temporally separating their individual fluorescence emission.




{kind=link}