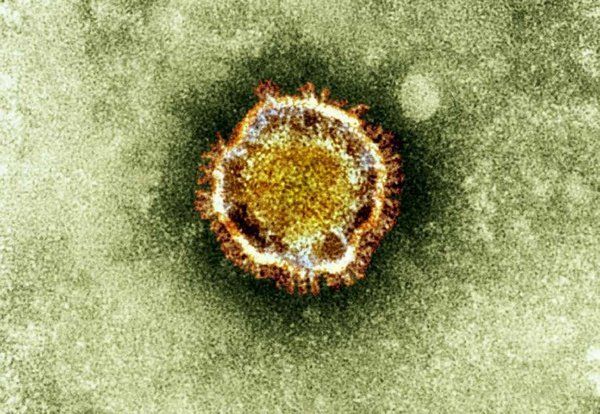
ZURICH (Reuters) — Switzerland’s health care system could collapse by the end of the month if the new coronavirus keeps spreading at current rates, a government official warned on Tuesday.
Swiss authorities estimated that 2,650 people had tested positive for the coronavirus and said 19 people had died, while predicting cases will likely soar in the weeks ahead.
Exact figures were unavailable. Daniel Koch, head of the Federal Office of Health’s communicable diseases division, said the rapid rise had outstripped the state’s ability to record new cases in real time.
Sam Harris discusses the coronavirus withAmesh Adalja.
In this episode of the podcast, Sam Harris speaks with Amesh Adalja about the spreading coronavirus pandemic. They discuss the contagiousness of the virus and the severity of the resultant illness, the mortality rate and risk factors, vectors of transmission, how long coronavirus can live on surfaces, the importance of social distancing, possible anti-viral treatments, the timeline for a vaccine, the importance of pandemic preparedness, and other topics.
Amesh Adalja, MD, is an infectious disease specialist at the Johns Hopkins University Center for Health Security. His work is focused on emerging infectious disease, pandemic preparedness, and biosecurity. Amesh has served on US government panels tasked with developing guidelines for the treatment of plague, botulism, and anthrax. He is an Associate Editor of the journal Health Security, co-editor of the volume Global Catastrophic Biological Risks, and a contributing author for the Handbook of Bioterrorism and Disaster Medicine. Amesh actively practices infectious disease, critical care, and emergency medicine in the Pittsburgh metropolitan area.
Francisco Garcia, a youth team coach at Malaga-based club Atletico Portada Alta, had an unknown pre-existing health condition that resulted in him being more vulnerable to the virus than usual for an individual of his age, though he was only informed of having cancer after going to hospital with symptoms of coronavirus.
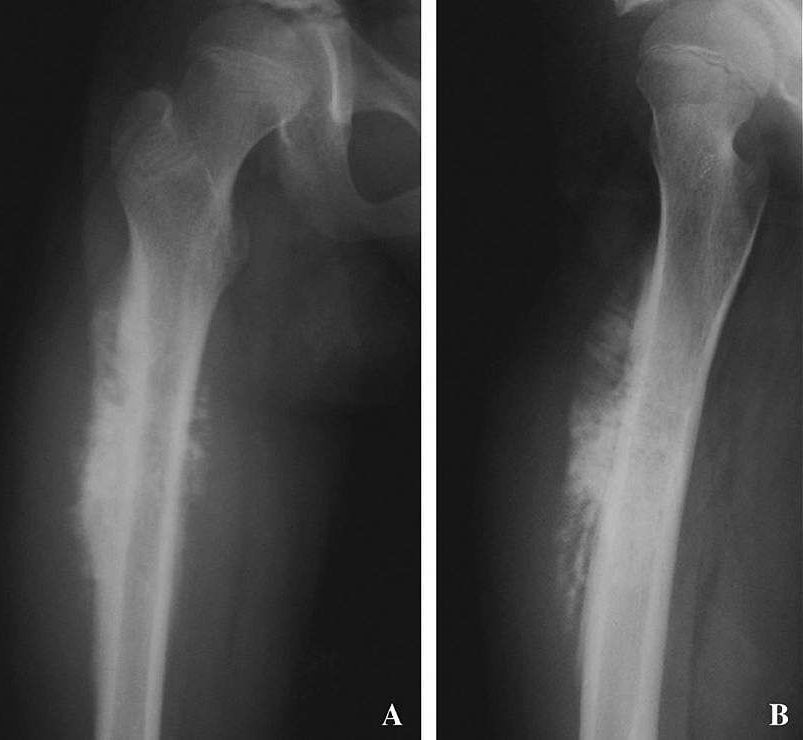
A study by researchers at the National Cancer Institute (NCI), part of the National Institutes of Health, offers new insight into genetic alterations associated with osteosarcoma, the most common cancerous bone tumor of children and adolescents. The researchers found that more people with osteosarcoma carry harmful, or likely harmful, variants in known cancer-susceptibility genes than people without osteosarcoma. This finding has implications for genetic testing of children with osteosarcoma, as well as their families.
The study was published March 19, 2020, in JAMA Oncology.
“With this study, we wanted to find out how many people with osteosarcoma may have been at high risk for it because of their genetics,” said Lisa Mirabello, Ph.D., of NCI’s Division of Cancer Epidemiology and Genetics (DCEG), who led the research. “We not only learned that at least a quarter of the people in the study with osteosarcoma had a variant in a gene known to predispose someone to cancer, we also uncovered variants that had never before been associated with this cancer.”
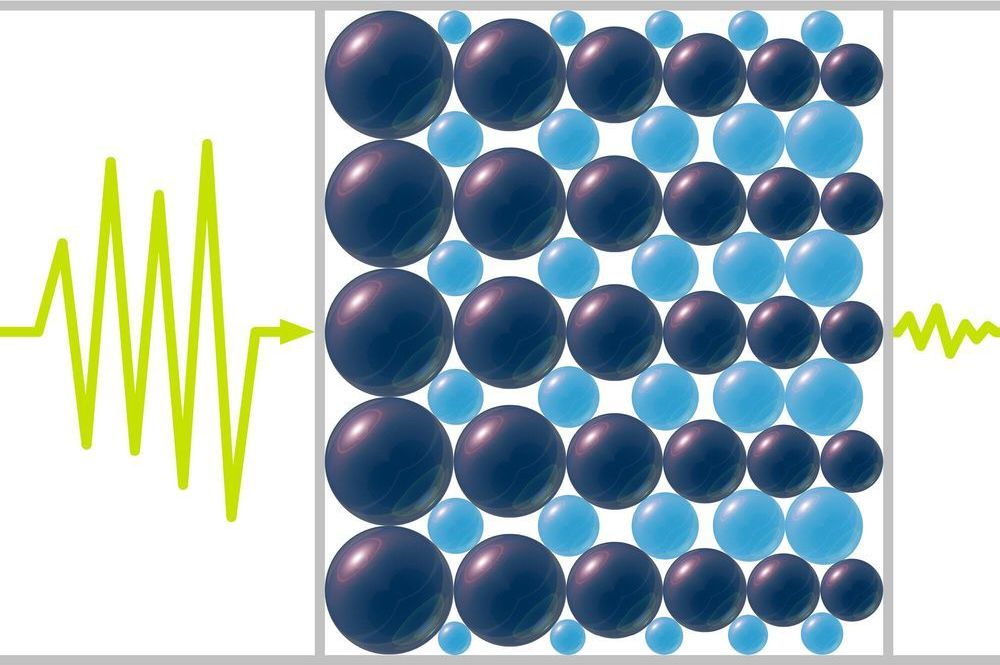
Need to reduce high-pitched noises? Science may have an answer.
In a new study, theoretical physicists report that materials made from tapered chains of spherical beads could help dampen sounds that lie at the upper range of human hearing or just beyond.
The impacts of such noises on health are uncertain. But some research suggests that effects could include nausea, headaches, dizziness, impaired hearing or other symptoms.
The U.S. Health and Human Services Department suffered a cyberattack on its computer system Sunday night during the nation’s response to the coronavirus pandemic, according to three people familiar with the matter.
The attack appears to have been intended to slow the agency’s systems down, but didn’t do so in any meaningful way, said the people, who asked for anonymity to discuss an incident that was not public.
The National Security Council tweeted just before midnight: “Text message rumors of a national #quarantine are FAKE. There is no national lockdown. @CDCgov has and will continue to post the latest guidance on #COVID19.”
Chinese officials say they’ll have a coronavirus vaccine ready next month for emergency situations and clinical trials.
Eight institutes in the country are working on five approaches to inoculations in an effort to combat COVID-19, according to the South China Morning Post. The contagious illness has sickened more than 118,000 people and killed at least 4,200 worldwide, mostly in mainland China, as of Tuesday afternoon.
“According to our estimates, we are hopeful that in April some of the vaccines will enter clinical research or be of use in emergency situations,” Zheng Zhongwei, director of the National Health Commission’s Science and Technology Development Center, said Friday.
Scientists can now edit multiple sites in the genome at the same time to learn how different DNA stretches co-operate in health and disease.
CRISPR-based DNA editing has revolutionized the study of the human genome by allowing precise deletion of any human gene to glean insights into its function. But one feature remained challenging—the ability to simultaneously remove multiple genes or gene fragments in the same cell. Yet this type of genome surgery is key for scientists to understand how different parts of the genome work together in the contexts of both normal physiology and disease.
Now such a tool exists thanks to the teams of Benjamin Blencowe and Jason Moffat, both professors of molecular genetics at the Donnelly Centre for Cellular and Biomolecular Research. Dubbed ‘CHyMErA’, for Cas Hybrid for Multiplexed Editing and Screening Applications, the method can be applied to any type of mammalian cell to systematically target the DNA at multiple positions at the same time, as described in a study published in the journal Nature Biotechnology.
Disaster emergency is in response to the global COVID-19 pandemic and the effects it is having on the city.
The City of Boulder has declared a local disaster emergency in response to the global COVID-19 pandemic and the effects it is having on the city.
City Manager Jane Brautigam issued a disaster emergency declaration today effective at 6 p.m. This creates a state of emergency for Boulder. The declaration provides the city manager with tools necessary to protect the public health and safety. The City Manager has authority to issue a disaster emergency declaration for a period of up to 7 days. To be effective for more than 7 days, the declaration must be confirmed and extended by the city council. Staff will ask the city council to consider doing so at the March 17, 2020 council meeting. The disaster emergency declaration provides the city manager with the authority to, among other things, order a curfew, limit large gatherings, close streets and sidewalks and order businesses to close. Violation of any emergency order would be punishable by a fine of up to $1000 and up to 90 days in jail.
Coronavirus’s economic danger is exponentially greater than its health risks to the public. If the virus does directly affect your life, it is most likely to be through stopping you going to work, forcing your employer to make you redundant, or bankrupting your business.
The trillions of dollars wiped from financial markets this week will be just the beginning, if our governments do not step in. And if President Trump continues to stumble in his handling of the situation, it may well affect his chances of re-election. Joe Biden in particular has identified Covid-19 as a weakness for Trump, promising “steady, reassuring” leadership during America’s hour of need.