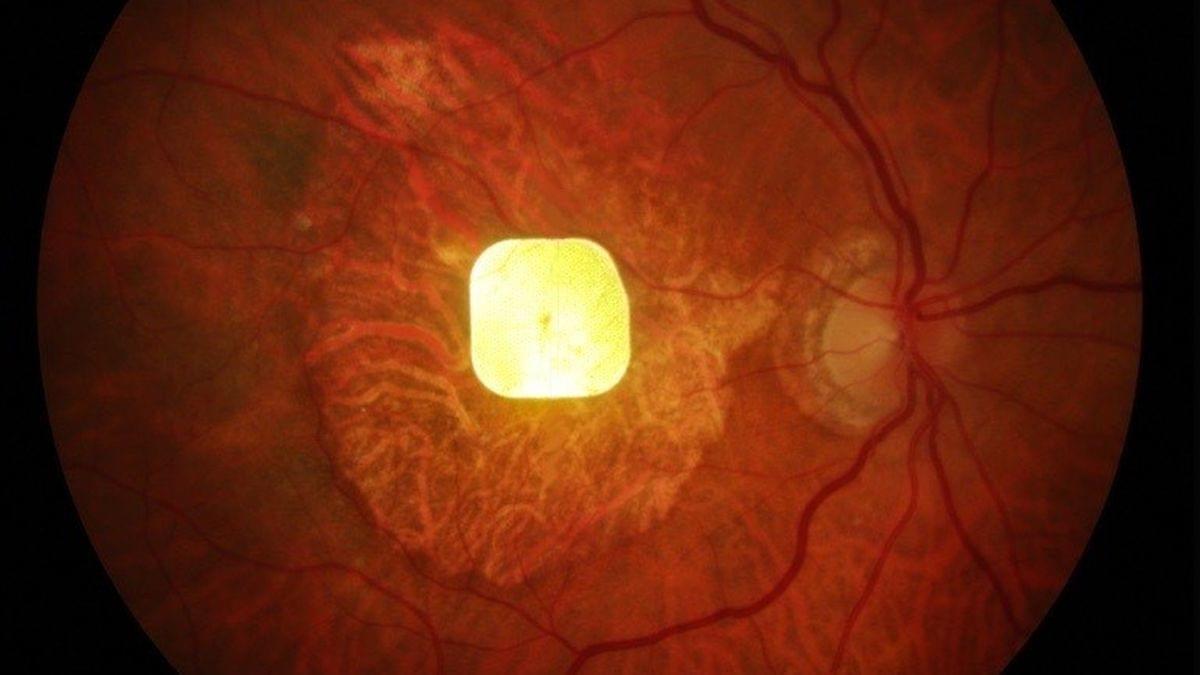
A tiny chip implanted into the eyes of people suffering vision loss from irreversible age-related macular degeneration has restored central sight in a dazzling first.
It’s called the PRIMA system, tested across 17 European hospitals, and it restored central vision in 26 of 32 patients who used it for 12 months – many of whom could even read again. The result, developed by a large international team of doctors and scientists over many years, represents a massive breakthrough in treatments for vision loss.
“It’s the first time that any attempt at vision restoration has achieved such results in a large number of patients,” says ophthamologist José-Alain Sahel of the University of Pittsburgh School of Medicine, co-senior author on a paper describing the results.