Vision is one of the most crucial human senses, yet more than 300 million people worldwide are at risk of vision loss due to various retinal diseases. While recent advancements in retinal disease treatments have successfully slowed disease progression, no effective therapy has been developed to restore already lost vision—until now.
KAIST researchers led by Professor Jinwoo Kim from the Department of Biological Sciences have successfully developed a novel drug to restore vision through retinal nerve regeneration. The research is published in the journal Nature Communications. The study was co-authored by Dr. Eun Jung Lee of Celliaz Inc. and Museong Kim, a Ph.D. candidate at KAIST, as joint first authors.
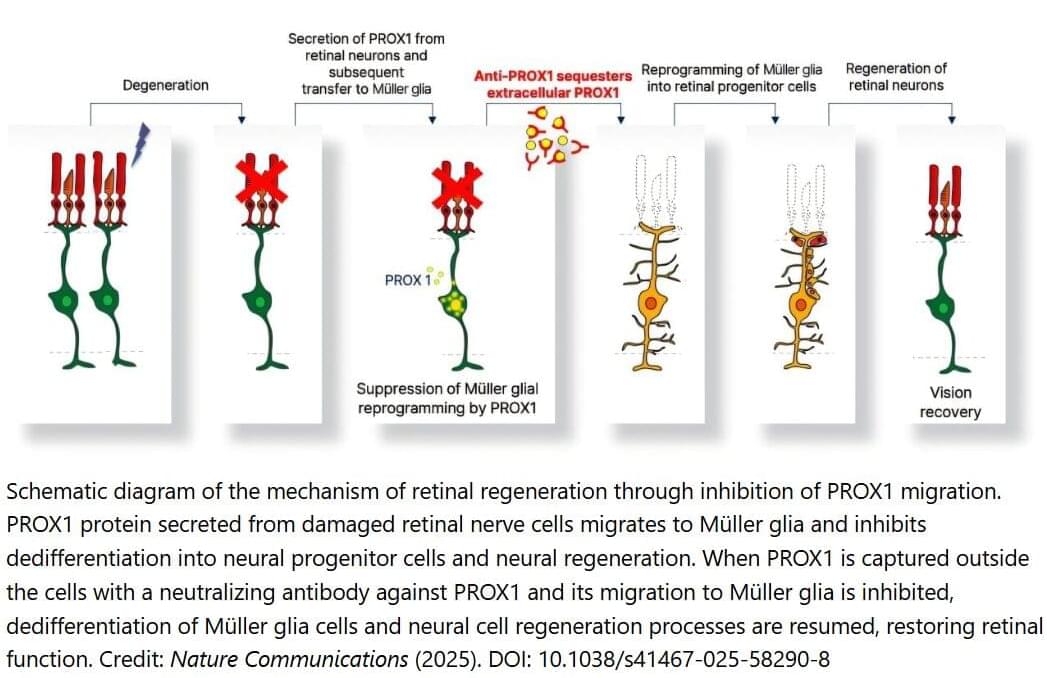
The research team successfully induced neural regeneration and vision recovery in a disease-model mouse by administering a compound that blocks the PROX1 (Prospero Homeobox 1) protein, which suppresses retinal regeneration. The effect lasted for more than six months.