A new study from researchers at Tyndall National Institute and the National University of Singapore shows that subtle changes in the intermolecular van der Waals interactions in the active component of a molecular diode can improve the device performance by more than a factor of ten.
A team of scientists from Tyndall National Institute at University College Cork and the National University of Singapore have designed and fabricated ultra-small devices for energy-efficient electronics. By finding out how molecules behave in these devices, a ten-fold increase in switching efficiency was obtained by changing just one carbon atom. These devices could provide new ways to combat overheating in mobile phones and laptops, and could also aid in electrical stimulation of tissue repair for wound healing. The breakthrough creation of molecular devices with highly controllable electrical properties will appear in the February issue of Nature Nanotechnology. Dr. Damien Thompson at the Tyndall National Institute, UCC and a team of researchers at the National University of Singapore led by Prof. Chris Nijhuis designed and created the devices, which are based on molecules acting as electrical valves, or diode rectifiers.
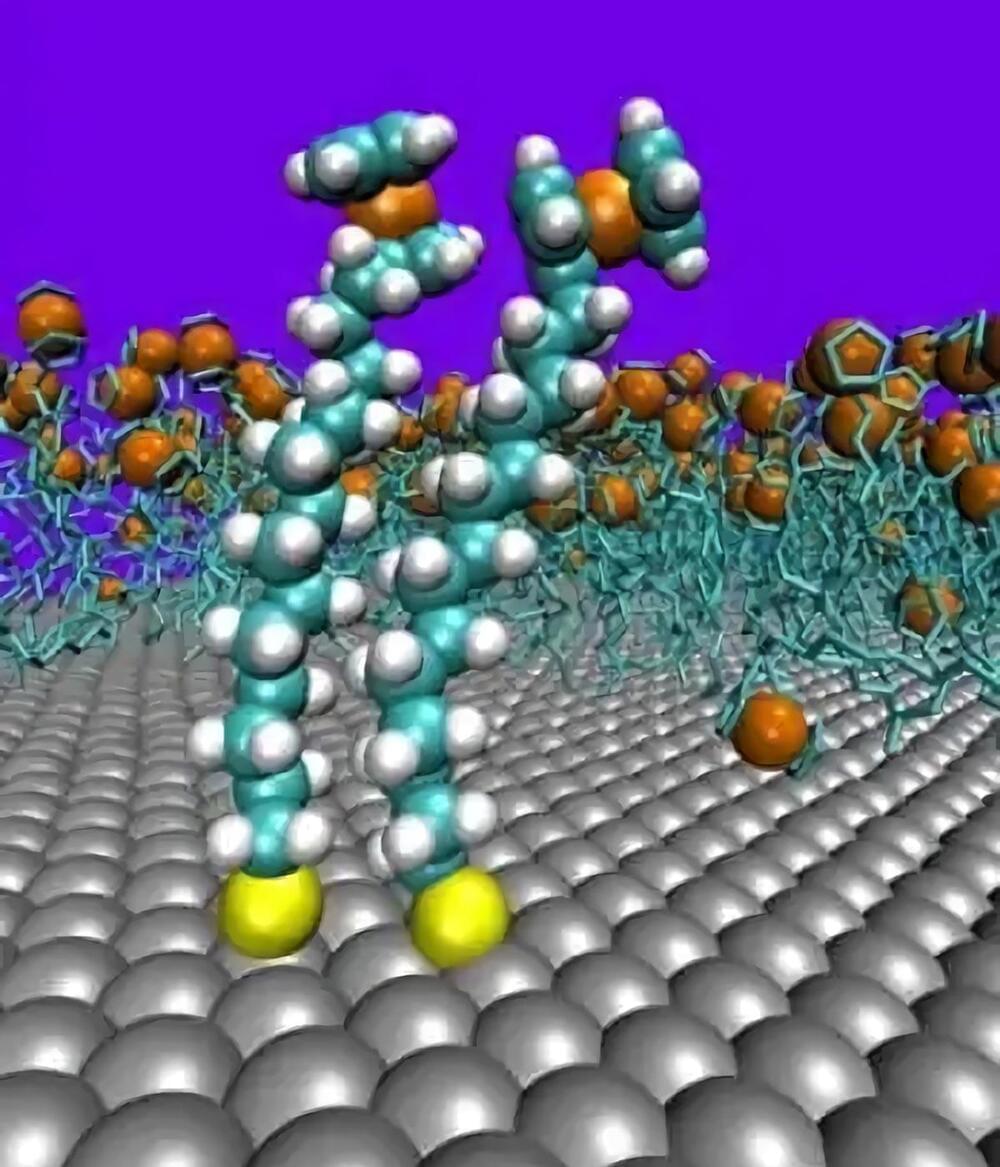
Dr. Thompson explains “These molecules are very useful because they allow current to flow through them when switched ON and block current flow when switched OFF. The results of the study show that simply adding one extra carbon is sufficient to improve the device performance by more than a factor of ten. We are following up lots of new ideas based on these results, and we hope ultimately to create a range of new components for electronic devices.” Dr. Thompson’s atom-level computer simulations showed how molecules with an odd number of carbon atoms stand straighter than molecules with an even number of carbon atoms. This allows them to pack together more closely. Tightly-packed assemblies of these molecules were formed on metal electrode surfaces by the Nijhuis group in Singapore and were found to be remarkably free of defects. These high quality devices can suppress leakage currents and so operate efficiently and reliably.