The potential threat of biological warfare with a specific agent is proportional to the susceptibility of the population to that agent. Preventing disease after exposure to a biological agent is partially a function of the immunity of the exposed individual. The only available countermeasure that can provide immediate immunity against a biological agent is passive antibody. Unlike vaccines, which require time to induce protective immunity and depend on the host’s ability to mount an immune response, passive antibody can theoretically confer protection regardless of the immune status of the host. Passive antibody therapy has substantial advantages over antimicrobial agents and other measures for postexposure prophylaxis, including low toxicity and high specific activity. Specific antibodies are active against the major agents of bioterrorism, including anthrax, smallpox, botulinum toxin, tularemia, and plague. This article proposes a biological defense initiative based on developing, producing, and stockpiling specific antibody reagents that can be used to protect the population against biological warfare threats.
Defense strategies against biological weapons include such measures as enhanced epidemiologic surveillance, vaccination, and use of antimicrobial agents, with the important caveat that the final line of defense is the immune system of the exposed individual. The potential threat of biological warfare and bioterrorism is inversely proportional to the number of immune persons in the targeted population. Thus, biological agents are potential weapons only against populations with a substantial proportion of susceptible persons. For example, smallpox virus would not be considered a useful biological weapon against a population universally immunized with vaccinia.
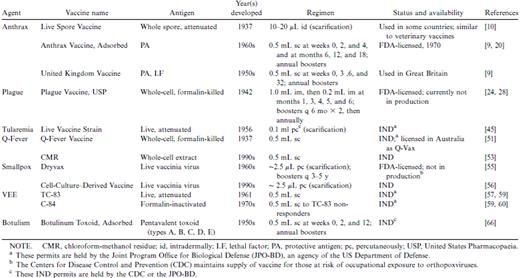
Vaccination can reduce the susceptibility of a population against specific threats provided that a safe vaccine exists that can induce a protective response. Unfortunately, inducing a protective response by vaccination may take longer than the time between exposure and onset of disease. Moreover, many vaccines require multiple doses to achieve a protective immune response, which would limit their usefulness in an emergency vaccination program to provide rapid prophylaxis after an attack. In fact, not all vaccine recipients mount a protective response, even after receiving the recommended immunization schedule. Persons with impaired immunity are often unable to generate effective response to vaccination, and certain vaccines may be contraindicated for them.