Google Assistant has been our go-to assistant for years, and now a new directive from Google might make it better than ever with Bard integration.

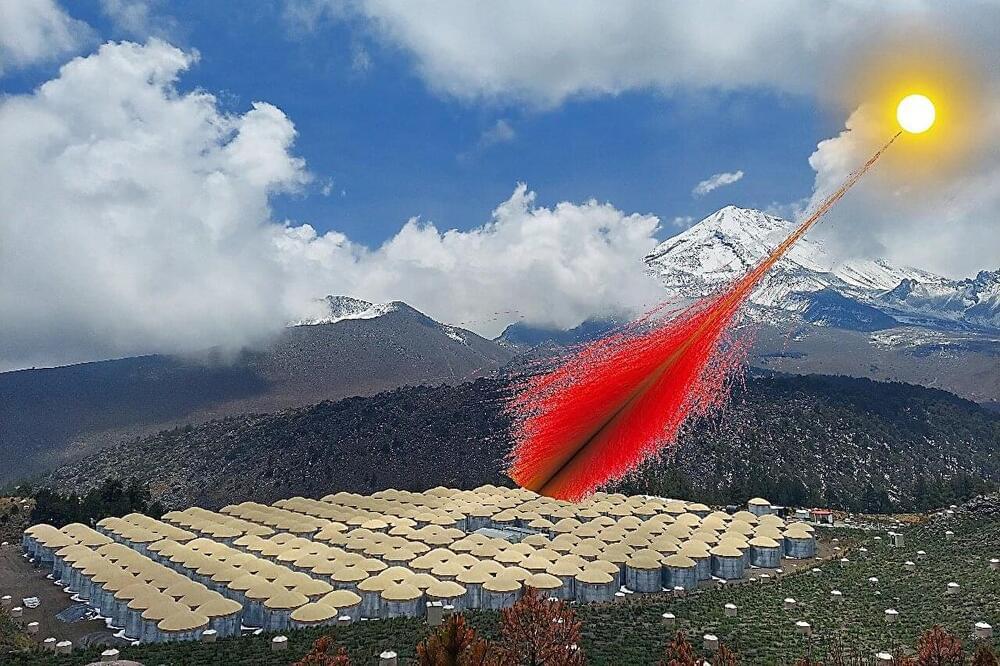
Sometimes, the best place to hide a secret is in broad daylight. Just ask the sun.
“The sun is more surprising than we knew,” said Mehr Un Nisa, a postdoctoral research associate at Michigan State University. “We thought we had this star figured out, but that’s not the case.”
Nisa, who will soon be joining MSU’s faculty, is the corresponding author of a new paper in the journal Physical Review Letters that details the discovery of the highest-energy light ever observed from the sun.




The skin is the largest organ of the body, comprising several compartments and about 20 different cell types that are involved in various skin functions – complexity that is more than skin deep! [1] Skin aging is a multifactorial process that is impacted by several intrinsic and extrinsic factors. Constant exposure of the human skin to such stimuli impacts its function and accelerates aging resulting in dry skin, wrinkling, thinning of the epidermis, and reduced barrier integrity. While we notice most of those changes by looking in a mirror – something the cosmetics industry has leveraged to multi-billion dollar effect – older skin is more at risk of injury, less able to sense touch, heat and cold, slower to heal and more prone to cellulitis and other skin infections.
Aging is a complex and gradual process characterized by a reduction in function and reproducibility along with an increase in the incidence of degenerative diseases. Skin aging has been reported to be associated with the presence and accumulation of senescent cells. “A number of diseases that increase in older people may have a unifying underlying mechanism having to do with senescence,” says Ruth Montgomery, PhD, professor of medicine and epidemiology (microbial diseases) at Yale School of Medicine [2].
Senescent cells are those that have lost their proliferative capacity, are resistant to apoptosis, and secrete factors that can cause tissue deterioration and inflammation [3]. These factors are termed senescence-associated secretory phenotype (SASP) and can lead to extracellular matrix (ECM) deposition, impact epidermal stem cell renewal and worsen melanin synthesis.

Scientists at Purdue University are propelling the future of robotics and autonomous systems forward with their patent-pending method that improves typical machine vision and perception.
Zubin Jacob, the Elmore Associate Professor of Electrical and Computer Engineering in the Elmore Family School of Electrical and Computer Engineering, and research scientist Fanglin Bao have developed HADAR, or heat-assisted detection and ranging. Their research was featured on the cover of the July 26 issue of the peer-reviewed journal Nature.
Jacob said it is expected that one in 10 vehicles will be automated and that there will be 20 million robot helpers that serve people by 2030.
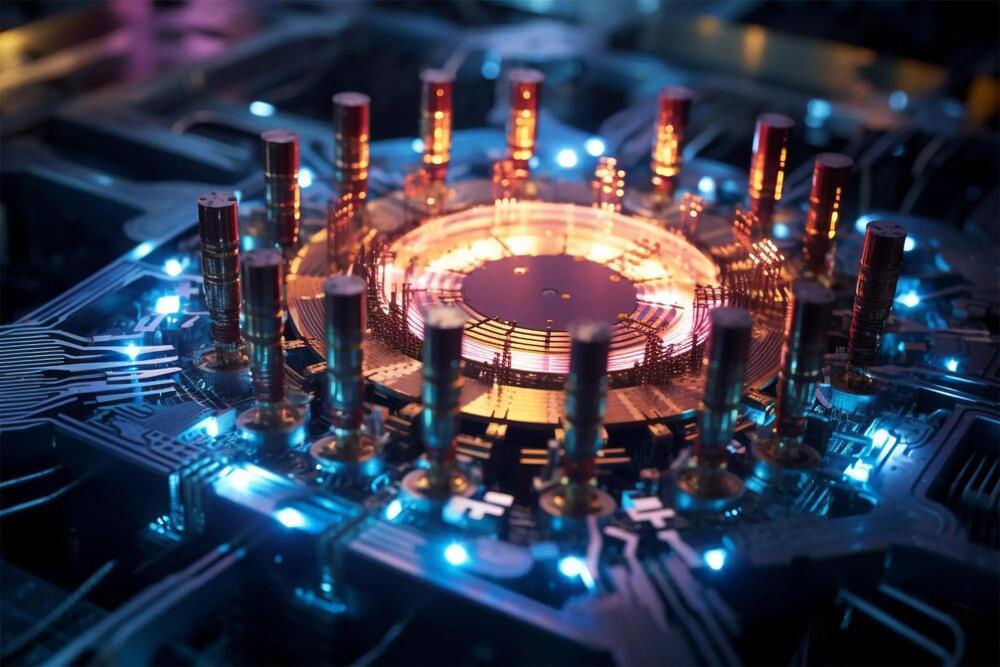
A German-Chinese research team has successfully created a quantum bit in a semiconductor nanostructure. Using a special energy transition, the researchers created a superposition state in a quantum dot – a tiny area of the semiconductor – in which an electron hole simultaneously possessed two different energy levels. Such superposition states are fundamental for quantum computing.
Previously, the induction of such a state necessitated a large-scale, free-electron laser capable of emitting light in the terahertz range. Unfortunately, this wavelength was too long to accurately focus the beam on the quantum dot. This team, however, achieved the excitation with two carefully calibrated, short-wavelength optical laser pulses.
The team headed by Feng Liu from Zhejiang University in Hangzhou, together with a group led by Dr. Arne Ludwig from Ruhr University Bochum and other researchers from China and the UK, report their findings in the journal Nature Nanotechnology, published online on July 24, 2023.
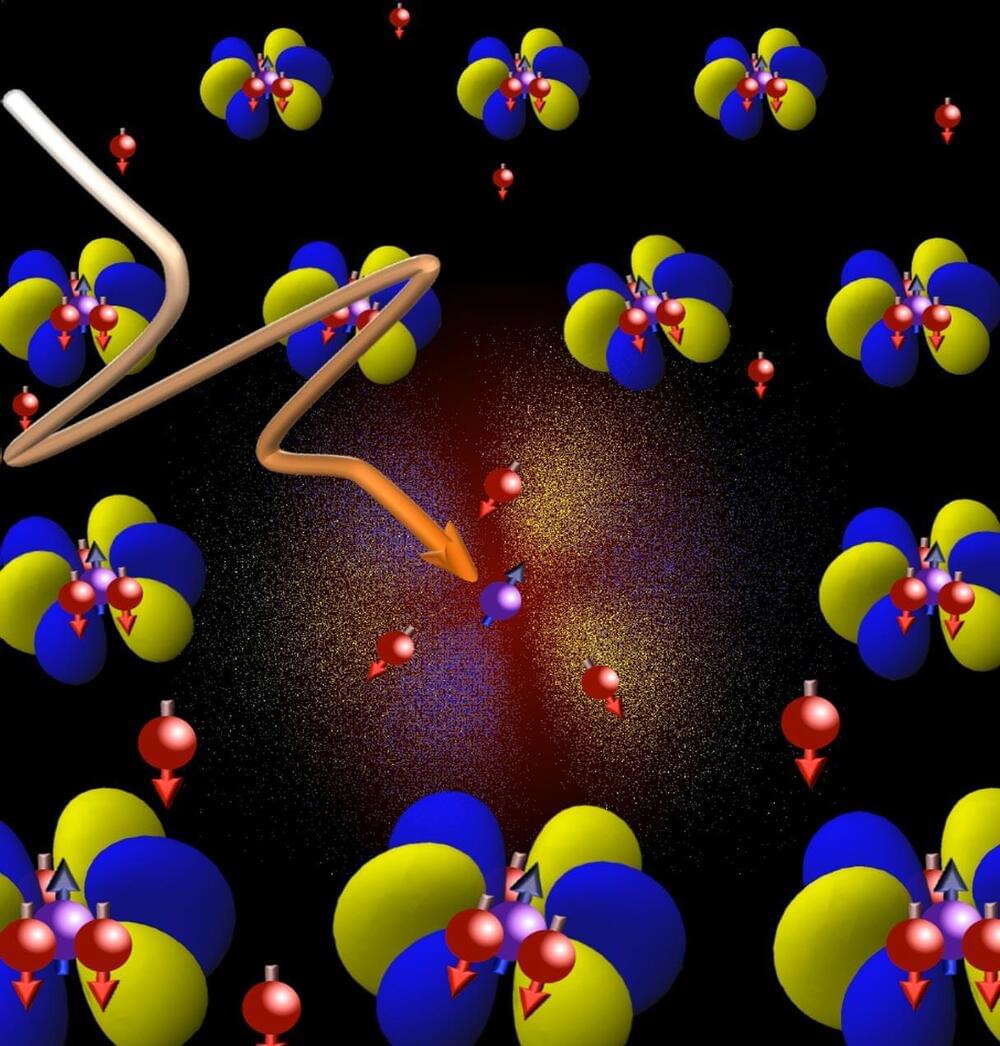
Scientists observe an effect in the quantum world that does not exist in the macrocosm.
Researchers at the University of Bonn and ETH Zurich have conducted an in-depth study of unique phase transitions in certain metals. Their findings provide a better understanding of quantum physics and potentially advance the field of quantum information technology.
When they are cooled below a certain critical temperature, many substances change their properties. For example, such a phase transition occurs, when water freezes. However, in certain metals, there are phase transitions that do not exist in the macrocosm. They arise because of the special laws of quantum mechanics that apply in the realm of nature’s smallest building blocks. It is thought that the concept of electrons as carriers of quantized electric charge no longer applies near these exotic phase transitions.

Each cell in the body stores its genetic information in DNA in a stable and protected form that is readily accessible for the cell to carry on its activities. Nevertheless, mutations—changes in genetic information—occur throughout the human genome and can have a powerful influence on human health and evolution.
“Our team is interested in a classical question about mutation—why do mutation rates in the genome vary so tremendously from one DNA location to another? We just do not have a clear understanding of why this occurs,” said Dr. Md. Abul Hassan Samee, assistant professor of integrative physiology at Baylor College of Medicine and corresponding author of the work.
Previous studies have shown that the DNA sequences flanking a mutated position—the sequence context—play a strong role in the mutation rate. “But this explanation still leaves unanswered questions,” Samee said. “For example, one type of mutation occurs frequently in a specific sequence context while a different type of mutation occurs infrequently in that same sequence context. So, we think that a different mechanism could explain how mutation rates vary in the genome. We know that each building block or base that makes up a DNA sequence has its own 3D chemical shape. We proposed, therefore, that there is a connection between DNA shape and mutations rates, and this paper shows that our idea was correct.”