All my links: https://linktr.ee/daveshap
Join us on Patreon! https://www.patreon.com/MichaelLustgartenPhD
Discount Links/Affiliates:
Blood testing (where I get the majority of my labs): https://www.ultalabtests.com/partners/michaellustgarten.
At-Home Metabolomics: https://www.iollo.com?ref=michael-lustgarten.
Use Code: CONQUERAGING At Checkout.
Clearly Filtered Water Filter: https://get.aspr.app/SHoPY
Epigenetic, Telomere Testing: https://trudiagnostic.com/?irclickid=U-s3Ii2r7xyIU-LSYLyQdQ6…M0&irgwc=1
Use Code: CONQUERAGING
NAD+ Quantification: https://www.jinfiniti.com/intracellular-nad-test/
Meta claims its new models are superior to those from OpenAI and Google across ‘a broad range’ of benchmarks.

Meta claims its new models are superior to those from OpenAI and Google across ‘a broad range’ of benchmarks.
(/ ˈ m ʌr i ˈ ɡ ɛ l ˈ m æ n / ; September 15, 1929 – May 24, 2019) [ 3 ] [ 4 ] [ 5 ] [ 6 ] was an American theoretical physicist who played a preeminent role in the development of the theory of elementary particles. Gell-Mann introduced the concept of quarks as the fundamental building blocks of the strongly interacting particles, and the renormalization group as a foundational element of quantum field theory and statistical mechanics. He played key roles in developing the concept of chirality in the theory of the weak interactions and spontaneous chiral symmetry breaking in the strong interactions, which controls the physics of the light mesons. In the 1970s he was a co-inventor of quantum chromodynamics (QCD) which explains the confinement of quarks in mesons and baryons and forms a large part of the Standard Model of elementary particles and forces.
Murray Gell-Mann received the 1969 Nobel Prize in Physics for his work on the theory of elementary particles.
![]()
Official code implementation for ‘Graph Low-Rank Adapters of High Regularity for Graph Neural Networks and Graph Transformers’ — PanPapag/GConv-Adapter

Carbon locked in soils can be emitted by bacteria. Turning up the heat on them releases more carbon.
Gestational diabetes is a disorder characterized by abnormally high levels of blood glucose (also called blood sugar) during pregnancy.
Affected women do not have diabetes before they are pregnant, and most of these women go back to being nondiabetic soon after the baby is born. Gestational diabetes is often discovered during the second trimester of pregnancy.
The disease has a 30 to 70 percent chance of recurring in subsequent pregnancies.
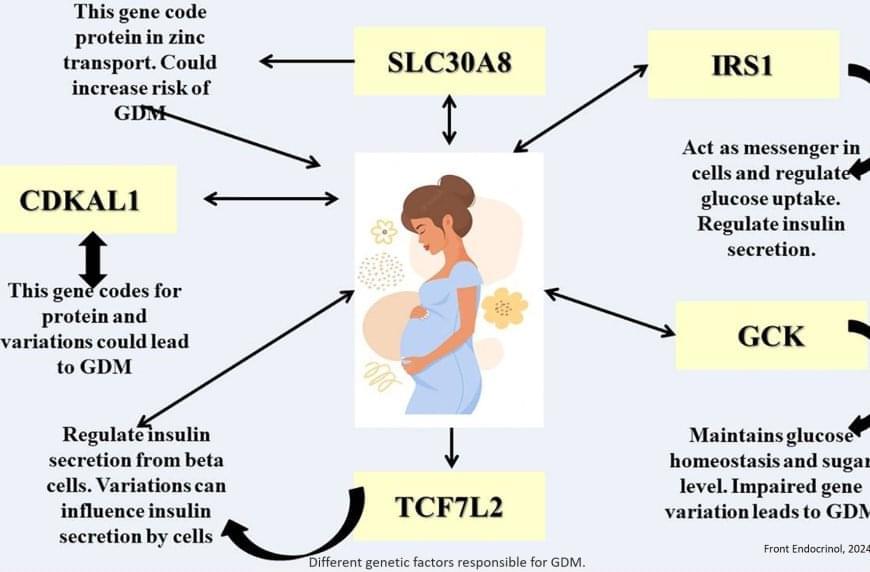
Gestational diabetes mellitus (GDM) is influenced by both genetic and environmental factors. Polymorphisms in genes related to glucose metabolism and insulin signaling, such as TCF7L2, have been associated with increased risk. This gene influences insulin secretion and glucose production, affecting the body’s ability to regulate blood sugar during pregnancy. Other implicated genes include GCK, encoding glucokinase, and MTNR1B, involved in melatonin receptor signaling.
More information on genetic factors that contribute to the development of GDM is provided in the link below.
Posted in biotech/medical, genetics, robotics/AI | Leave a Comment on Sensory Processing Challenges in Children with Neurodevelopmental Disorders and Genetic Conditions: An Observational Study
A variety of genetic conditions are known to affect brain development and, consequently, might potentially exhibit behaviours related to SIDs, as they impact areas involved in sensory processing and the perceptual integration of inputs. This is the case of Williams syndrome (WS), 22q11.2 deletion syndrome (22qDS) and pseudohypoparathyroidism (PHP). Although some previous research indicates sensory processing alterations in WS [20], this area remains largely unexplored in 22qDS and PHP.
The condition 22qDS, caused by a deletion in the q11.2 region of chromosome 22, is associated with significant brain abnormalities, along with cardiac anomalies, cleft palate, immune deficiencies, cognitive difficulties, and an increased risk of psychiatric disorders such as schizophrenia [21]. Common structural alterations include hypoplasia of the corpus callosum, which impacts interhemispheric communication, and anomalies in the thalamus, affecting the relay of sensory and motor information. Additionally, structural changes in the cortical brain regions, such as variations in cortical thickness, have been observed. These structural abnormalities are linked to disruptions in neural networks and can contribute to deficits in cognitive and emotional functions, impacting development and behaviour in individuals with the syndrome [22].
WS is caused by a microdeletion in the chromosomal region 7q11.23. It is characterised by a distinctive cognitive and behavioural profile, including strong social and verbal skills, accompanied by anxiety and attention problems. Additionally, individuals with WS may present with cardiovascular anomalies, hypercalcemia in infancy, and a distinctive facial phenotype [23]. MRI studies reveal reduced brain size and a more pronounced loss of white matter compared to grey matter in WS. The posterior brain regions are notably more affected, with reduced grey matter density observed in the superior parietal lobe and hypofunction near the intraparietal sulcus, areas associated with multisensory integration and perception [24].