Author(s): Towards AI Team Introduction Continue reading on Towards AI » Published via Towards AI.

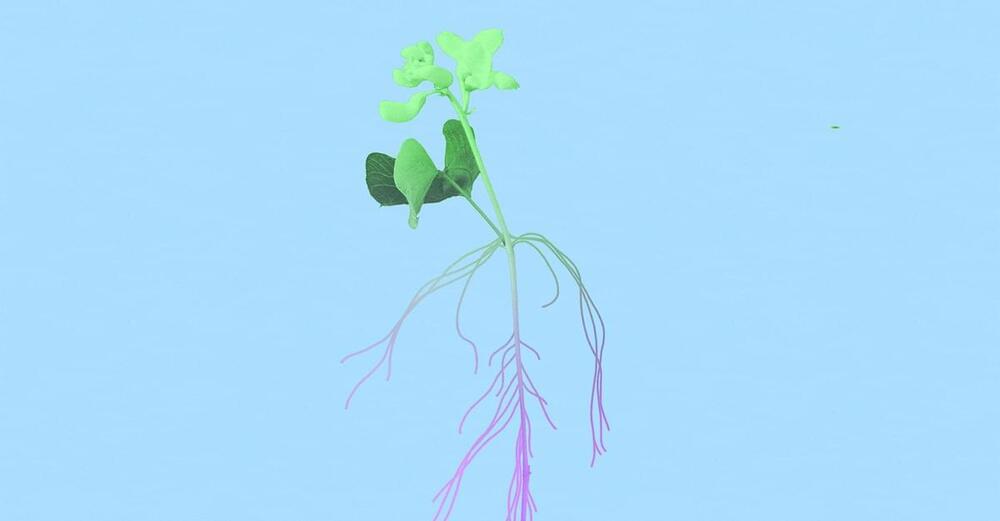
Scientists are debating whether concepts such as memory, consciousness, and communication can be applied beyond the animal kingdom, Zoë Schlanger wrote in our June 2024 issue.
“Consciousness was once seen as belonging solely to humans and a short list of nonhuman animals that clearly act with intention,” Schlanger wrote in an article adapted from her book, “The Light Eaters: How the Unseen World of Plant Intelligence Offers a New Understanding of Life on Earth.”
“Yet seemingly everywhere researchers look, they are finding that there is more to the inner lives of animals than we ever thought possible. Scientists now talk regularly about animal cognition; they study the behaviors of individual animals, and occasionally ascribe personalities to them. Some scientists now posit that plants should likewise be considered intelligent.”
“Not so long ago, treading even lightly in this domain could upend a scientist’s career,” Schlanger continued. The popular 1973 book “The Secret Life of Plants” included real science, but also featured wildly unscientific projection; many scientists were unable to reproduce its claims, Schlanger wrote, causing a decades-long avoidance of plant-behavior studies.
A decade later, a paper by David Rhoades, a zoologist and chemist at the University of Washington, proposed that trees were communicating with one another to defend against a caterpillar infestation. Rhoades was ridiculed by peers; his discovery ended up buried, even as it opened new lines of inquiry. “Four decades on, the idea that plants might communicate intentionally with one another remains a controversial concept in botany,” Schlanger wrote. Definitions of communication are slippery; intentionality is even harder to show.
The essential question of plant intelligence is “How does something without a brain coordinate a response to stimuli?” Schlanger continued. “How does information about the world get translated into action that benefits the plant? How can the plant sense its world without a centralized place to parse that information?” To learn more, she spoke with scientists studying plant agency, memory, and other avenues of research.

Join us on Patreon! https://www.patreon.com/MichaelLustgartenPhD
Discount Links/Affiliates:
Blood testing (where I get the majority of my labs): https://www.ultalabtests.com/partners/michaellustgarten.
At-Home Metabolomics: https://www.iollo.com?ref=michael-lustgarten.
Use Code: CONQUERAGING At Checkout.
Clearly Filtered Water Filter: https://get.aspr.app/SHoPY
Epigenetic, Telomere Testing: https://trudiagnostic.com/?irclickid=U-s3Ii2r7xyIU-LSYLyQdQ6…M0&irgwc=1
Use Code: CONQUERAGING
NAD+ Quantification: https://www.jinfiniti.com/intracellular-nad-test/
Entire atoms have been put through a classic quantum experiment for the first time and the breakthrough could lead to better detectors for picking up the gravitational waves that ripple across the universe.
By Alex Wilkins
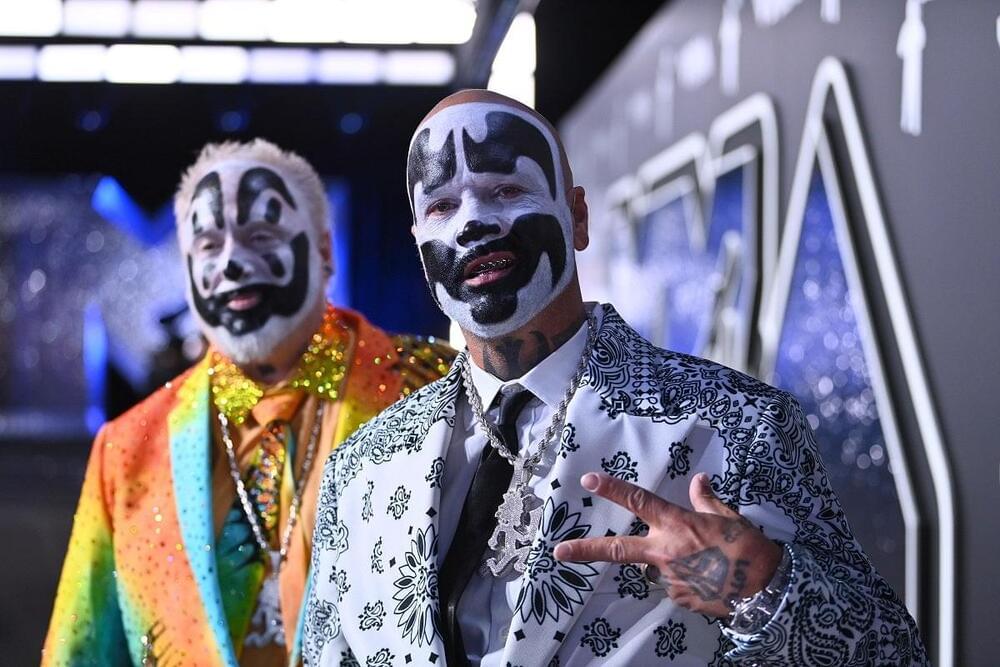
Insane Clown Posse’s Joseph Utsler, better known by his stage persona Shaggy 2 Dope, has an AI clone — and apparently, he’s a fan.
Hosted on the Google-backed Character. AI service — which, as a sidebar, Futurism has investigated extensively, repeatedly finding horrible things — the ICP cofounder’s digital doppelganger sounds like a slightly robotic version of the real thing.
The effect is so uncanny that Mr. Dope himself decided to hit the AI up and bring it onto his livestreamed vlog, “The Shaggy Show.”
Researchers developed a “waveform movement” technology enabling robots to express emotions through natural facial gestures.
While these earthquakes are not impacting Kilauea, one of the world’s most active volcanoes, it has been intermittently erupting since Dec. 23.
According to the latest update from the Hawaiian Volcano Observatory, the intensity of these eruptions, so-called “lava fountaining,” has strengthened after weakening in the days after the initial eruption.
Webcam observations by USGS scientists show that these eruptions are currently confined to its crater.

Scientists are challenging the existence of dark energy with a new model called “timescape,” which suggests the Universe’s expansion might be influenced by its uneven structure rather than an invisible force.
This theory could resolve ongoing cosmological debates, with upcoming satellite data playing a key role in confirming its validity.
Questioning Dark Energy’s Existence