{kind=link}
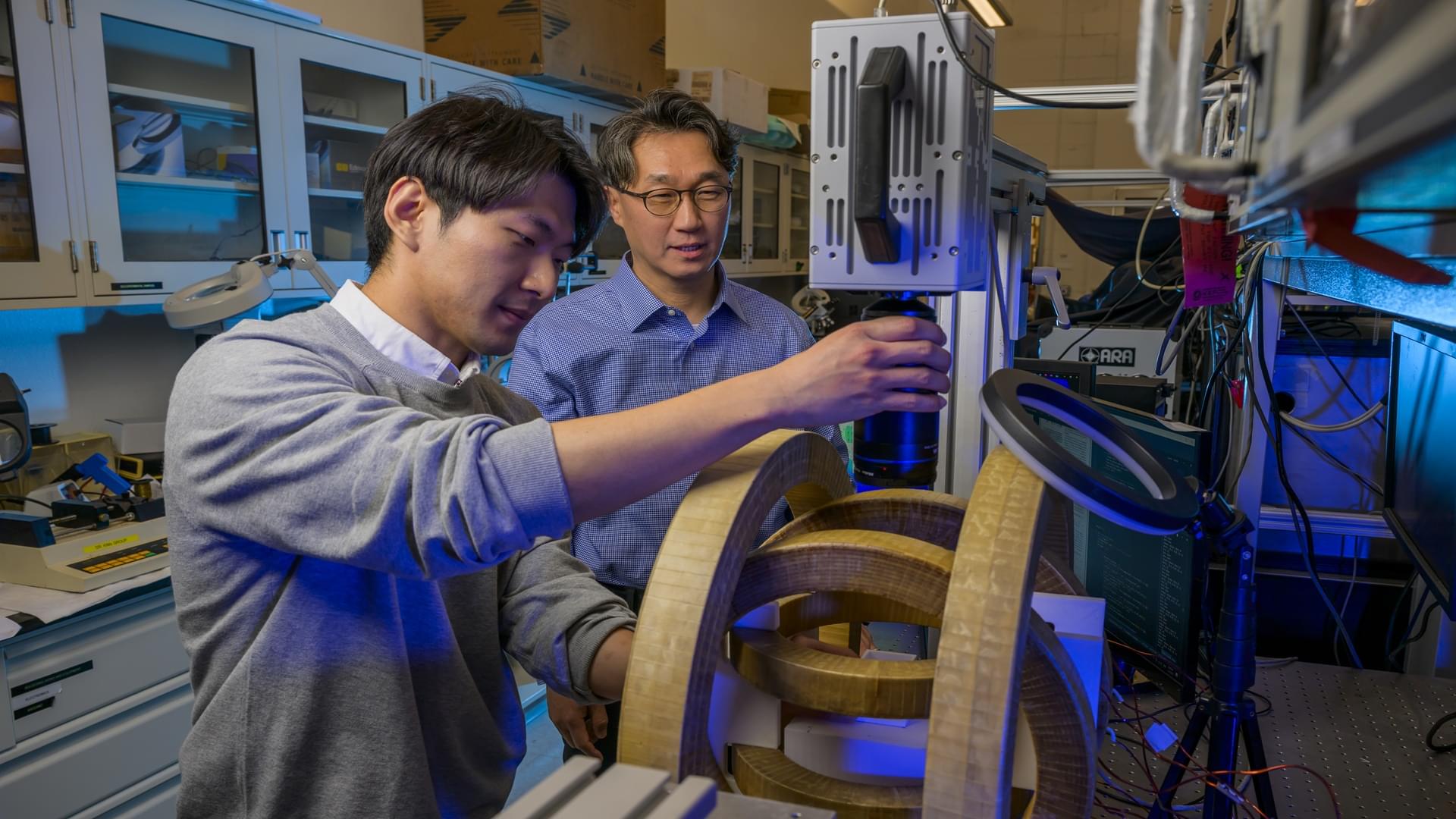
New SMU system controls microrobots without cameras, enabling use in hard-to-see environments like the human body.
Get the latest international news and world events from around the world.


{kind=link}

Alzheimer’s Risk Gene Alters Brain Activity Early — But It May Be Reversible
Carrying one or two copies of the APOE4 gene variant significantly increases the risk of developing Alzheimer’s, and a new study reveals how APOE4 can change neuron activity – potentially many years before symptoms such as memory loss start showing.
In young mice bred to have the APOE4 gene, researchers found specific neurons were smaller and more hyperactive in parts of the brain’s memory center, the hippocampus.
What’s more, they were able to identify a protein, Nell2, contributing to the disruption – and a potential pathway to reverse the damage in advanced cases.

Living buildings are now a reality. Swiss scientists unveil a self-healing material that breathes
Can a wall get stronger the more it breaks, and greener the more it stands? Swiss scientists say buildings are about to start breathing and devouring carbon, and the concrete status quo will not like the math.
From a Zurich lab comes a building skin that inhales carbon, knits its own cracks and grows sturdier with time. Researchers at ETH Zurich embedded photosynthetic cyanobacteria in a 3D printed hydrogel, creating a living material that draws down CO₂ and strengthens over time, its chlorophyll tinting it green. Across 400 days of testing, a prototype matched the yearly uptake of a 20-year-old pine, pulling in up to 18 kilograms of CO₂, while each gram of the base material fixes about 26 milligrams. Detailed in Nature Communications on April 6, 2026 and co-authored by Mark Tibbitt, the work points to facades that do carbon duty as part of everyday architecture.
Some breakthroughs feel both surprising and oddly familiar, like rediscovering a tool nature kept in plain sight. Swiss scientists have blended biology with architecture to shape a new kind of material that lives with its surroundings. It repairs small cracks, it sips CO2 from the air, and it quietly strengthens with time. The promise is simple, and bold: buildings that help clean the sky.